

INTRODUCTION
Spine fracture represents a substantial global health burden, contributing significantly to disability, chronic pain management challenges, functional impairment, and substantial healthcare expenditures1,2. Epidemiological data indicate a rising global incidence of these fractures. For instance, Finnish population registries documented a 57% increase in spine fracture hospitalization rates between 1998 and 2017, rising from 57 to 89 cases per 100000 person3. Similarly, German health statistics reported a 45.6% surge in spine fracture incidence from 2009 to 2019, reaching 150.7 cases per 100000 population4. The significant morbidity and economic impact associated with these injuries underscore the critical need for effective preventive strategies and early detection methods.
Tobacco consumption remains a leading preventable cause of global mortality and morbidity. Despite substantial progress in tobacco control initiatives, approximately 1.3 billion individuals worldwide continue to use tobacco products, resulting in over 7 million annual deaths attributable to tobacco-related diseases5. In developed nations, the mortality burden primarily manifests through malignancies (lung, upper digestive tract, bladder), chronic obstructive pulmonary disease, and cardiovascular disorders6. Both direct smoking and secondhand smoke inhalation have demonstrated detrimental effects on skeletal health. Mechanistic studies indicate that tobacco smoke disrupts normal bone remodeling cycles, promoting accelerated bone loss and osteoporosis development, thereby increasing fracture susceptibility7. Beyond initial fracture risk, tobacco users experience compromised bone healing capacity and delayed fracture union, with some skeletal impairments persisting for years following cessation8. Current epidemiological evidence specifically addressing the tobacco-spine fracture relationship remains limited and inconclusive. Cotinine, the primary nicotine metabolite with superior pharmacokinetic properties, including an extended half-life and consistent metabolic clearance, provides a highly reliable exposure biomarker. Consequently, serum cotinine measurement represents the gold standard for quantifying tobacco smoke exposure in biomedical research9.
The present study aims to comprehensively evaluate the association between biologically quantified tobacco smoke exposure and spine fracture prevalence through a secondary analysis of cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) 1999–2010, 2013–2014, 2017–2020. By extending these epidemiological observations, we seek to enhance understanding of tobacco’s skeletal effects and inform evidence-based fracture prevention strategies.
METHODS
Data sources and study population
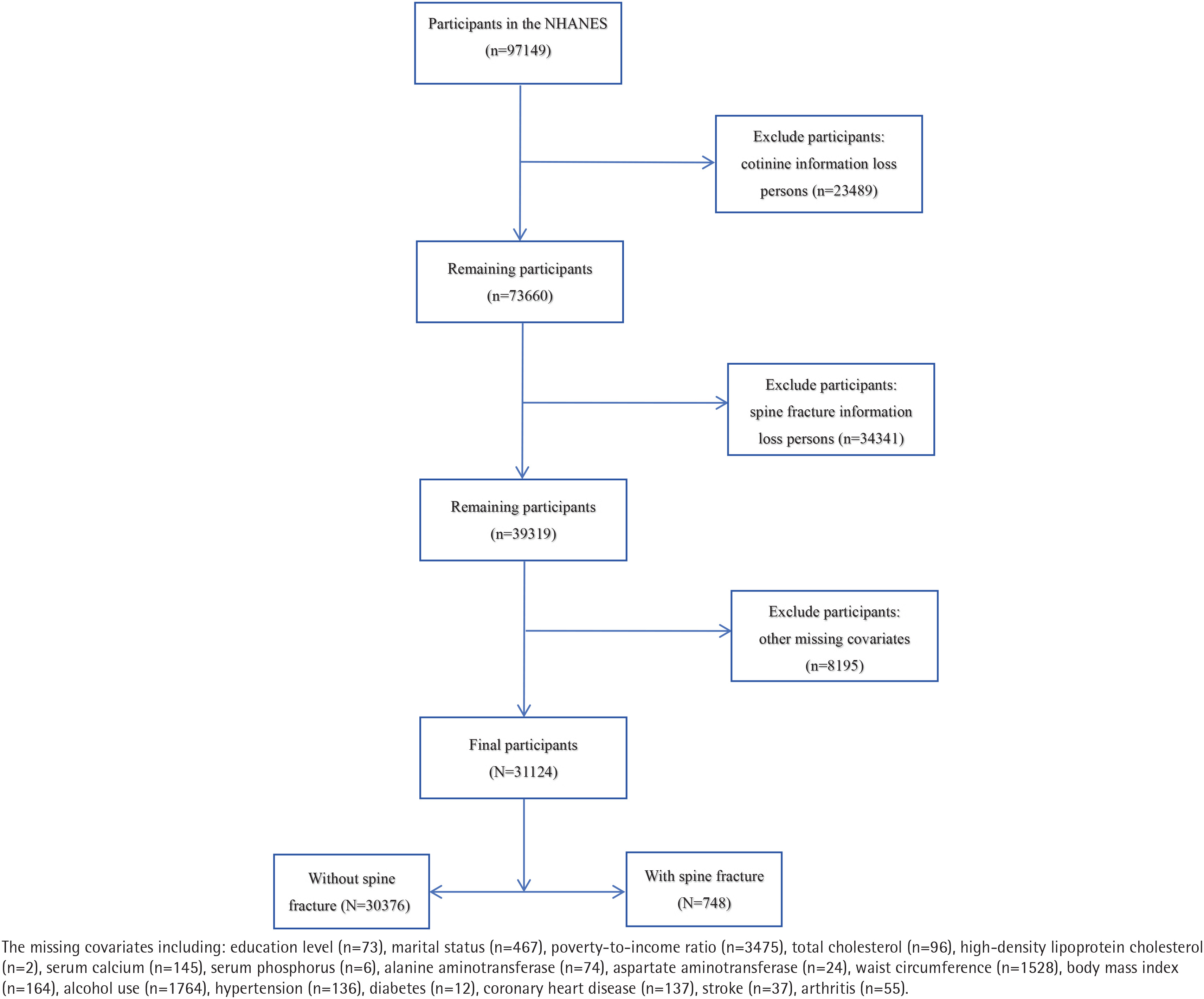
The analysis drew on nationally representative data from the National Health and Nutrition Examination Survey (NHANES)10, a comprehensive study conducted by the National Center for Health Statistics (NCHS) that evaluates the health and nutritional status of children and adults in the United States. A multistage, probability-based sampling strategy is employed in the survey to ensure that the derived estimates accurately reflect the target population10. The NHANES survey protocol was reviewed and approved by the National Center for Health Statistics (NCHS) Institutional Review Board. All participants provided written informed consent. As the present study constitutes a secondary analysis of de-identified, publicly available data, it was exempt from additional ethical review by an institutional review board. This research was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki, while reporting standards followed the STROBE checklist for cross-sectional studies. We aggregated data from eight survey cycles (1999–2000, 2001–2002, 2003–2004, 2005–2006, 2007–2008, 2009–2010, 2013–2014, 2017–2020), initially identifying 97149 potential participants aged ≥20 years. After sequentially excluding individuals with missing cotinine measurements (n=23489), undetermined fracture status (n=34341), and incomplete covariate data (n=8195), our final analytical sample comprised 31124 participants (Figure 1).
Assessment of tobacco smoke exposure
Tobacco smoke exposure was assessed by measuring serum cotinine, which serves as a proxy for both direct inhalation and passive inhalation of environmental tobacco smoke11. The analytical method involved isotope-dilution high-performance liquid chromatography/atmospheric pressure chemical ionization tandem mass spectrometry (ID HPLC-APCI MS/MS). The analytical capacity of this method includes a lower limit of detection of 0.015 ng/mL and an intra-assay coefficient of variation (CV) of <10%. These technical specifications ensure high precision and reliability in quantifying serum cotinine levels. For categorical analysis, we adopted the cut-point recommended by Benowitz et al.12 to define exposure levels: concentrations <0.05 ng/mL were classified as ‘Unexposed’; 0.05–2.99 ng/mL indicated ‘Low exposure’ from passive smoking; and levels ≥3 ng/mL identified ‘Heavy exposure’ consistent with active smoking.
Spine fracture definition
Spine fracture was operationalized as a self-reported, physician-diagnosed event, based on the following NHANES interview question from the Medical Conditions section: ‘Has a doctor or other health professional ever told you that you had a fracture or broken bone in your spine?’. Participants who responded ‘Yes’ were classified as having a spine fracture; those responding ‘No’ or ‘Don’t know’ were classified as non-cases. This epidemiological criterion for case identification has demonstrated adequate authenticity and is considered a feasible method in large-scale population studies, consistent with previous findings13.
Covariables data extraction
The NHANES protocol involved two primary data-collection modalities: standardized household interviews and comprehensive physical examinations conducted in mobile examination centers. Covariates for this analysis were selected a priori based on their established relevance in the scientific literature and clinical rationale. The set of adjustment variables encompassed demographic factors (age, gender, marital status, race/ethnicity, education level, family income), existing medical conditions (hypertension, diabetes, coronary heart disease [CHD], stroke, arthritis), anthropometric measurements (waist circumference [WC], body mass index [BMI]), behavioral factors (alcohol use), and a panel of serum biomarkers (total cholesterol [TC, mmol/L], high-density lipoprotein cholesterol [HDL-C, mmol/L], calcium [mg/dL], phosphorus [mg/dL], alanine aminotransferase [ALT, U/L], aspartate aminotransferase [AST, U/L], blood urea nitrogen [BUN, mg/dL], and uric acid [UA, mg/dL]). Marital status was dichotomized as married/cohabitating or living alone. Self-reported race/ethnicity was categorized as Non-Hispanic White, Non-Hispanic Black, Mexican American, or Other. Education level was divided into three groups: <9, 9–12, and >12 years. Family income level was determined using the poverty income ratio (PIR) and classified as low (PIR ≤ 1.3), medium (1.3< PIR ≤ 3.5), or high (PIR >3.5), consistent with federal guidelines14. The presence of comorbidities (hypertension, diabetes, CHD, stroke, arthritis) was ascertained via self-report of a prior physician diagnosis. Waist circumference was measured at the iliac crest using a standardized protocol. BMI was calculated as weight (kg) divided by height (m) squared and categorized as: underweight/normal <25, overweight 25–29.9, and obese ≥30 kg/m2 according to WHO criteria. Alcohol use was defined as the consumption of at least 12 alcoholic drinks in the past year, based on the NHANES Alcohol Use Questionnaire.
Weights processing
To account for the complex, multistage probability sampling design of NHANES and to produce nationally representative estimates, appropriate sample weights were applied in accordance with the NHANES analytical guidelines. Specifically, the weight variables used were WTMEC4YR (for 1999–2000 and 2001–2002), WTMEC2YR (for 2003–2004, 2005–2006, 2007–2008, 2009–2010, 2013–2014), and WTMECPRP (for 2017–2020). To create a single, analyzable weight for the combined dataset spanning all cycles, we followed the standard procedure recommended by the National Center for Health Statistics (NCHS). The weighting methodology proceeded as follows: initial standardization of raw weights within each survey period, followed by merging of standardized weights across multiple cycles to create a composite weight, which was then incorporated into all analytical models to produce estimates generalizable to the non-institutionalized US population15.
Statistical analysis
Our secondary analysis of publicly available data employed distribution-appropriate statistical approaches. Continuous variables with normal distributions are reported as means ± SD; non-normal variables as medians (IQR); and categorical variables as frequencies and percentages. Intergroup comparisons utilized ANOVA (normal), Kruskal-Wallis (non-normal), or chi-squared (categorical) tests. The distribution of serum cotinine violated normality assumptions, necessitating a natural log transformation prior to treating it as a continuous variable in sensitivity analyses.
To quantify the relationship between tobacco smoke exposure and spine fracture risk, we computed odds ratios (ORs) with corresponding 95% confidence intervals (95% CIs) through multivariable logistic regression. We constructed four sequential models with progressive adjustment: Model 1 constituted a crude, unadjusted analysis; Model 2 incorporated sociodemographic confounders (age, gender, race, marital status, education level, and family income); Model 3 further adjusted for anthropometric and biochemical parameters (WC, BMI, TC, HDL-C, calcium, phosphorus, ALT, AST, BUN, UA); and Model 4 represented the fully adjusted model, additionally controlling for behavioral and clinical comorbidities (alcohol use, hypertension, diabetes, CHD, stroke, arthritis). The goodness-of-fit of the final multivariable logistic regression model was evaluated using the Hosmer-Lemeshow test. After adjusting for the covariates specified in Model 4, in the restricted cubic spline (RCS) analysis, we used 4 knots, a common choice that provides sufficient flexibility without overfitting in large datasets. The knots were placed at the 5th, 35th, 65th, and 95th percentiles of the natural log-transformed serum cotinine distribution, following standard recommendations for percentile-based knot placement to ensure stable estimates across the exposure range. The assessment of linearity versus non-linearity was conducted formally using the Wald test. This test evaluates the null hypothesis that the coefficients for all nonlinear spline terms are simultaneously equal to zero. A non-significant p-value supports a linear relationship. Furthermore, we also conducted extensive subgroup analyses. The subgroups used for stratification and interaction testing were predefined based on their established clinical relevance and potential as effect modifiers in previous literature. These included age (<40 vs ≥40 years), gender, race, marital status (married/partnered vs living alone), poverty-income ratio, alcohol use, hypertension, diabetes, CHD, stroke, and arthritis.
All data analyses were performed using R (version 4.2.1; The R Foundation) and Free Statistics software platforms (version 2.1.1). The study population characteristics were summarized using descriptive statistics. A two-tailed significance threshold of p<0.05 was employed for all inferential statistical tests.
RESULTS
Basic characteristics
Table 1 summarizes the baseline demographic and clinical characteristics of the 31124 participants in the final analysis, including 748 spine fracture cases (2.4%). Demographic data show a mean age of 52.7 years and 49.1% male representation. Notably, significant disparities were discernible across all measured covariates, spanning demographic, anthropometric, biochemical, and clinical domains, when comparing the different exposure categories.
Table 1
Baseline characteristics of participants in the cross-sectional study of tobacco smoke exposure and spine fracture in the US, NHANES 1999–2010 2013–2014, 2017–2020 (N=31124)
[i] All statistical analyses in Table 1 were weighted using sample weights provided by NHANES to ensure that the results are nationally representative. Continuous variables with normal distributions are reported as means ± SD; non-normal variables as medians (IQR); and categorical variables as frequencies and percentages. P-values were derived from ANOVA (normal) Kruskal-Wallis (non-normal) or chi-squared (categorical) tests for intergroup comparisons. PIR: poverty-to-income ratio. TC: total cholesterol. HDL-C: high-density lipoprotein cholesterol. ALT: alanine aminotransferase. AST: aspartate aminotransferase. BUN: blood urea nitrogen. UA: uric acid. WC: waist circumference. BMI: body mass index. CHD: coronary heart disease.
Univariable and multivariable logistic regression analyses
Preliminary univariable screening identified numerous variables significantly associated with spine fracture risk, including demographic factors, biochemical markers, and comorbidities (Supplementary file Table 1).
When treated as a continuous variable, univariable models showed that every unit increase in LN-transformed serum cotinine was associated with 5% higher odds of spine fracture (OR=1.05; 95% CI: 1.03–1.06). Table 2 presents the results of the multivariable logistic regression analysis examining the relationship between serum cotinine levels and spine fracture prevalence. After progressive adjustment (Model 4), the association remained robust: each unit increase in LN-cotinine corresponded to a 4% elevation in the odds of spine fracture (AOR=1.04; 95% CI: 1.02–1.06). We also performed a categorical analysis using the unexposed group (<0.05 ng/mL) as reference, which revealed a consistently elevated risk in the heavily exposed group (≥3 ng/mL). In contrast, the low exposure group (0.05–2.99 ng/mL) showed no significant association in any of the multivariable models (AOR=1.07; 95% CI: 0.87–1.30). The association for the heavy exposure group remained significant throughout the adjustment process, demonstrating odds ratios of 1.43 (95% CI: 1.21–1.69) in the crude model, 1.62 (95% CI: 1.35–1.95) after demographic adjustment, 1.60 (95% CI: 1.33–1.93) with additional biochemical/anthropometric adjustments, and 1.41 (95% CI: 1.16–1.70) in the fully adjusted model (Table 2).
Table 2
Multivariable logistic regression analysis the association between tobacco smoke exposure and spine fracture across different exposure levels in the US, NHANES 1999–2010, 2013–2014, 2017–2020 (N=31124)
[i] LN: natural logarithm. Model 1: unadjusted. AOR: adjusted odds ratio. Model 2: adjusted for age, gender, race, education level, marital status, PIR. Model 3: adjusted as in Model 2 plus TC, HDL-C, serum calcium, serum phosphorus, ALT, AST, BUN, UA, WC, BMI. Model 4: adjusted as in Model 3 plus alcohol use, hypertension, diabetes, CHD, stroke, arthritis.
Model fit assessment
The goodness-of-fit of the multivariable logistic regression model was assessed using the Hosmer-Lemeshow test. The results indicated that the model fit the data well, with a non-significant chi-squared value (χ2=4.091, df=8) (Table 3).
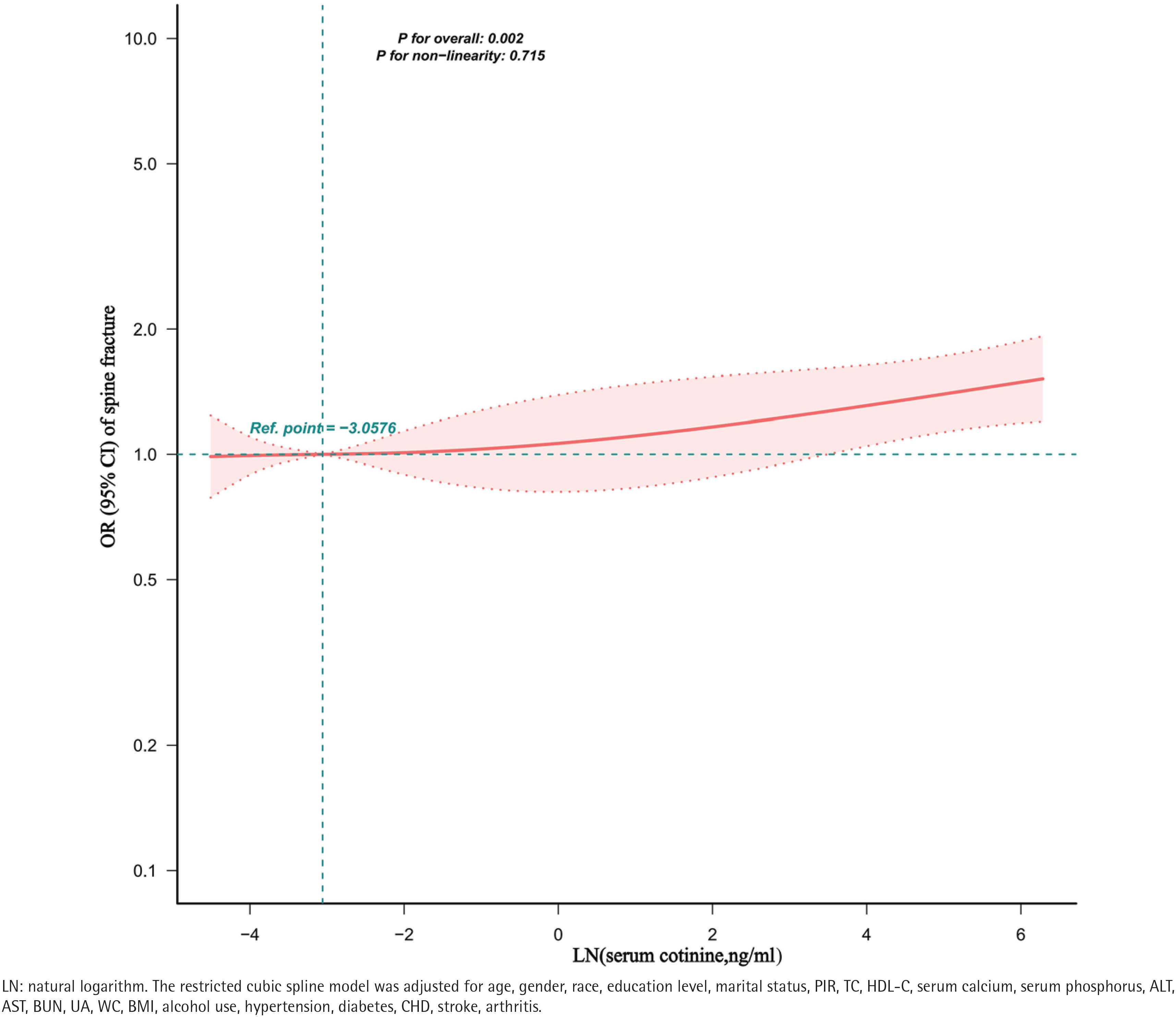
Restricted cubic spline models
The restricted cubic spline analysis revealed that the relationship between LN-cotinine and spine fracture prevalence was effectively linear, as indicated by a non-significant test for non-linearity. These results are consistent with a linear dose-response pattern without evident threshold effects (Figure 2).
Subgroup analysis
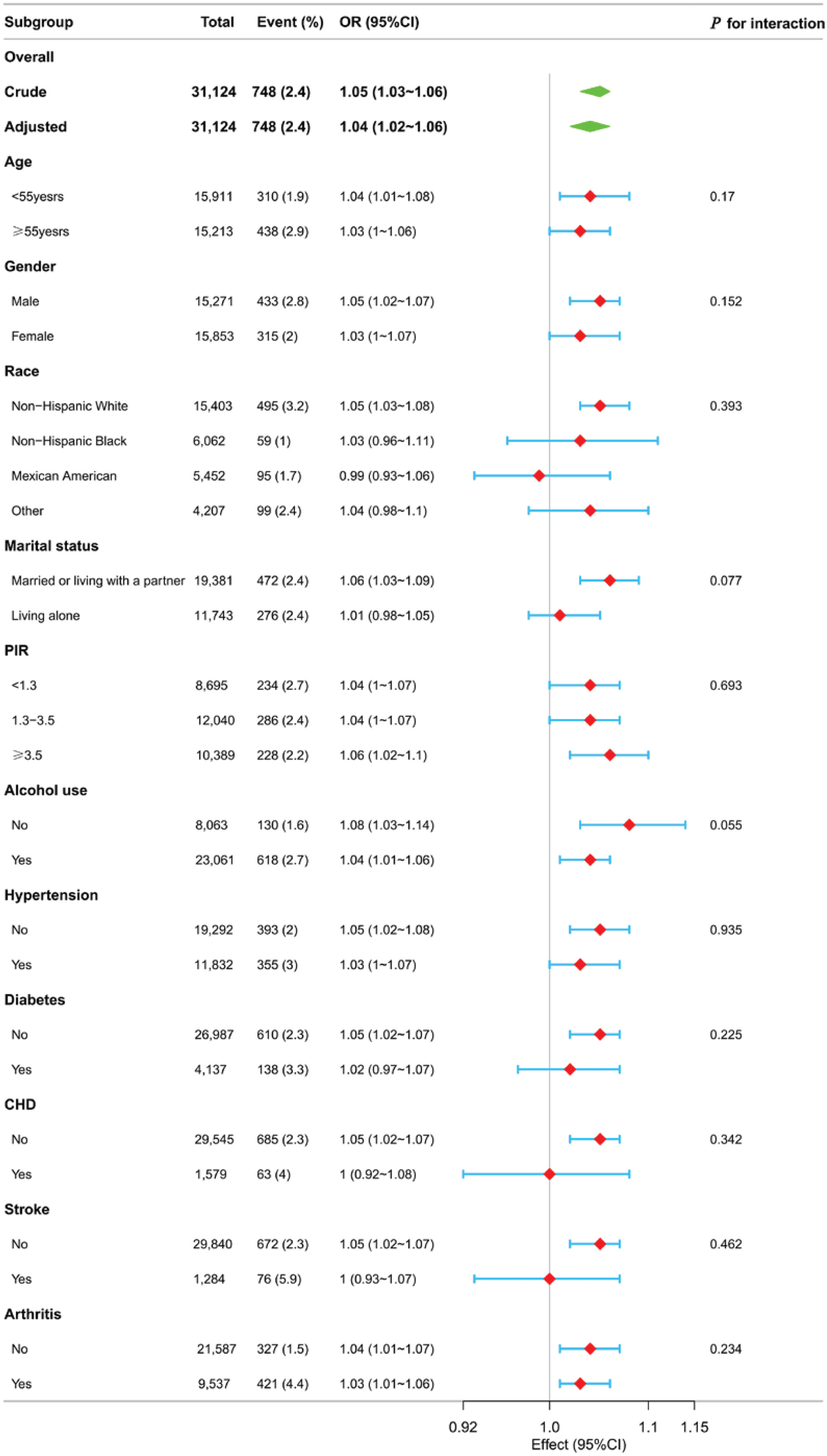
To evaluate the stability of the principal association, we performed extensive subgroup analyses stratified by age, gender, race, marital status, family income, alcohol use, and comorbidity status. Interaction testing revealed no significant effect modification by any of these stratification factors. The consistency of these results is visually presented in the forest plot (Figure 3) and detailed in Supplementary file Table 2.
DISCUSSION
In this large, nationally representative cross-sectional study of US adults, we identified a significant linear relationship between objectively measured tobacco smoke exposure and spine fracture risk after comprehensive adjustment for potential confounders. The data revealed a pattern in which higher serum cotinine concentrations were associated with progressively higher spine fracture prevalence, suggesting a dose-response relationship. Our modeling strategy, which involved four sequential levels of covariate adjustment, consistently demonstrated this positive association. Most notably, the fully adjusted model (Model 4) established a significant 41% increase in fracture odds for individuals in the highest exposure category (serum cotinine ≥3 ng/mL) compared to the unexposed group. This linear dose-response relationship was further corroborated by restricted cubic spline analysis, which revealed no evidence of threshold effects or non-linearity. Furthermore, the absence of significant effect modification in our extensive subgroup analyses suggests that the observed association is consistent across diverse demographic and clinical subgroups, reinforcing its robustness as a population-level risk factor. Collectively, these findings indicate that heavy tobacco smoke exposure, as quantified by serum cotinine, is substantially associated with a higher prevalence of spine fracture.
Previous research into the relationship between tobacco smoke exposure and spine fracture has been sparse. Prior investigations have discovered that smoking is connected to a significantly increased risk of fractures16,17. Specifically, in men, smoking boosts the risk of spine fracture to 32% and hip fracture to 40%18. Ampelas19 reviewed studies investigating the connection between smoking and hip fracture. The results showed that the incidence of hip fracture was elevated in current smokers19. Substantial biological evidence confirms that tobacco smoke disrupts bone remodeling homeostasis, predisposing individuals to reduced bone mineral density and clinical osteoporosis, which consequently elevates fracture susceptibility7. Beyond this elevated risk, tobacco users frequently encounter compromised bone healing capacity, with some skeletal impairments persisting long after cessation due to the prolonged nature of these pathological effects8. Critically, previous epidemiological investigations in this domain have been constrained by non-standardized smoking definitions and limited generalizability due to non-representative sampling. Our investigation addresses several key methodological limitations in the existing literature. It is noteworthy, however, that some prior studies have reported non-significant associations between smoking and fracture risk20,21. These discrepancies may be attributed to several methodological factors. First, many earlier studies relied on self-reported smoking status, which is susceptible to recall and social desirability bias, potentially leading to exposure misclassification and an underestimation of the true effect. Second, differences in study population characteristics (e.g. age, sex distribution, ethnicity, osteoporosis prevalence) and the extent of adjustment for key confounders (such as bone mineral density, physical activity, or corticosteroid use) may also contribute to heterogeneous findings. The present study, by utilizing an objective biomarker of tobacco exposure and a large, nationally representative sample with comprehensive covariate adjustment, helps to mitigate these limitations and provides a more robust estimate of the association. This study partially overcomes these limitations by utilizing objective biomarkers and nationally representative data. While our findings contribute to this field, further validation through trials is warranted to establish causality and elucidate the underlying biological mechanisms.
The elucidation of smoking’s role in fracture etiology remains incomplete, though research has identified several putative pathways that may mediate this relationship. One plausible mechanism linking smoking to fracture is the decline in bone mineral density (BMD) resulting from smoking22. Having a low BMD is the chief cause of the risk associated with osteoporotic fractures. It serves as a broadly applied indicator in clinical practice for recognizing patients who are more likely to sustain fractures23. Jing et al.24 have implicated ferroptosis activation as a critical pathway in tobacco toxin-induced osteoporosis, demonstrating that this process in bone marrow mesenchymal stem cells leads to impaired bone formation, characterized by accumulation of intracellular reactive oxygen species that activate AMPK signaling. In addition, Li et al.25 found, based on the Swedish Osteoporotic Fracture cohort study, that cadmium from smoking partly contributes to the risk of osteoporosis. Another possible mechanism is that smoking leads to a decrease in calcium absorption26, and changes in vitamin D metabolism result in a decrease in vitamin D levels in the blood27, leading to an increased risk of fracture. While future studies must clarify the causal nature of this association, our results nevertheless illuminate a significant and modifiable risk factor with substantial clinical relevance. Given the observed association between tobacco exposure and spine fracture, targeted interventions to reduce smoking and environmental nicotine exposure are essential. Based on the results of this study, it is evident that minimizing active smoking may be a crucial factor in addressing a modifiable factor associated with spine fracture.
Strengths and limitations
The nationwide and multi-ethnic scope of our study, based on the NHANES database with its complex sampling design, enhances the applicability and generalizability of our findings to the non-institutionalized US adult population. Furthermore, the large sample size (N=31124) provided adequate statistical power to detect the association of interest. In addition, a key methodological strength is the use of serum cotinine, an objective and quantitative biomarker, to assess tobacco smoke exposure. To our knowledge, this represents the first large-scale, population-based study to examine the specific relationship between tobacco smoke exposure (objectively measured by serum cotinine) and spine fracture risk. This approach minimizes misclassification bias inherent in self-reported smoking data and strengthens the internal validity of our exposure-outcome association. Finally, the application of complex survey weights in all analyses ensured that our estimates are representative of the non-institutionalized US adult population, further bolstering the external validity of our results.
However, several limitations should be noted. Firstly, the generalizability of our results may be constrained by the exclusive focus on the US population; external validation in diverse international cohorts is necessary. Secondly, the inherent constraints of the cross-sectional design preclude definitive causal inference regarding the relationship between tobacco smoke exposure and spine fracture. Thirdly, the assessment of serum cotinine at a single timepoint may not accurately reflect long-term exposure patterns, as it cannot account for intra-individual variability over time. Fourth, despite adjusting for a comprehensive set of covariates, residual confounding from unmeasured or imperfectly measured variables remains possible. Specifically, we lacked data on important potential confounders such as physical activity levels, dietary calcium and vitamin D intake, bone mineral density (BMD), history of falls, and use of medications affecting bone metabolism (e.g. glucocorticoids, bisphosphonates). Previous studies have identified these factors as significant predictors of fracture risk and may also be associated with smoking behavior, thus potentially confounding the observed association28. Fifth, the use of self-reported data for several variables, including spine fracture status and comorbidities, introduces the potential for recall bias and outcome misclassification. Finally, the exclusion of participants with missing data on cotinine, fracture status, or covariates (n=66025 excluded) may have introduced selection bias if these individuals differed systematically from those included in the analytical sample in terms of both exposure and outcome. Nevertheless, the large sample size and use of survey weights aim to mitigate the impact of this limitation on population-level inference.
CONCLUSIONS
This investigation provides evidence of a significant dose-response relationship between serum cotinine concentrations and spine fracture risk in US adults. Our results indicate that interventions aimed at reducing tobacco smoke exposure, particularly through smoking cessation, could be relevant for strategies aimed at reducing the population burden of these fractures. Additionally, serum cotinine measurement shows promise as a potential biomarker for stratifying individuals according to fracture risk. These findings extend the existing evidence base and underscore the importance of future prospective studies to confirm these observations and elucidate the underlying mechanisms.