
INTRODUCTION
In high-income settings, cardiovascular diseases and cancer have become the leading causes of death among people living with HIV (PLWH)1,2. Tobacco smoking is a major etiological factor for both diseases. High smoking prevalence among PLWH indicates a lack of effective smoking cessation interventions3.
Evidence from randomized clinical trials suggests that nicotine substitute products can improve quitting tobacco smoking and, therefore, reduce the associated health burden4. However, previous smoking cessation trials predominantly included people who were motivated to quit smoking and focused on testing a single nicotine substitution product5,6, which limits the clinical applicability of the results.
The Reduce tobacco use in people living with HIV in Switzerland (RETUNE) trial tests the effectiveness of offering a menu of nicotine substitute products, including e-cigarettes, nicotine pouches, and nicotine patches, on smoking cessation rate, to PLWH who smoke tobacco cigarettes regardless of their willingness to quit smoking (‘opt-out’ approach) (NCT06789692). RETUNE follows the Trials within Cohorts (TwiCs) design7. In TwiCs, participants first consent to the longitudinal data collection (cohort consent) and second, to be randomized into future trials (randomization consent). Participants who meet the eligibility criteria of a specific trial are then randomized. People in the control group are not informed about their allocation, while those randomized to the intervention group can accept or refuse the offered intervention, i.e. one of the products.
The objectives of this internal pilot study were to: 1) assess the acceptance rate of the offered intervention products among participants; 2) evaluate participants’ experiences with the intervention products in terms of satisfaction, handling, and side effects; and 3) refine the menu of offered products for the ongoing RETUNE trial.
METHODS
The reporting of this manuscript follows the CONSORT statement extension for pilot studies8.
RETUNE design
RETUNE is an ongoing, multicenter, pragmatic, 1:1 randomized, superiority clinical trial using the TwiCs design. Since 20 February 2025, we have been recruiting participants from the Swiss HIV Cohort Study (SHCS) at six participating hospitals (Basel, Zurich, St. Gallen, Bern, Geneva, Lausanne)9. The end of recruitment is estimated for December 2026.
The SHCS protocol (BASEC 2023-02080) and the RETUNE protocol, including the internal pilot study (BASEC 2024-02417), were approved by all involved ethics committees. All participants provided written cohort and randomization consent. The participants who accepted the intervention provided written informed consent.
Details on the trial design can be found in the protocol (Supplementary file Appendix 1). In brief, RETUNE includes participants aged ≥18 years, who signed the general SHCS randomization consent and smoke at least one tobacco cigarette per day. Pregnant women, as well as people who use e-cigarettes, nicotine pouches, or nicotine patches at trial start, are not eligible. The planned sample size of 972 participants was calculated under the assumption of a 50% acceptance rate of the offered intervention, i.e. participants selected an intervention product from the options provided. Eligibility is assessed automatically during routine cohort visits by an algorithm embedded in the SHCS database, which evaluates each participant’s current characteristics in real time. Eligible participants are then randomized by physicians using central randomization with minimization10. The physicians have no access to the random allocation sequence but are aware of the group assignment.
RETUNE interventions
Participants randomized to the control group receive usual care and are not informed about the RETUNE trial. Participants randomized to the intervention will be offered a menu of different nicotine substitute products in addition to usual care: e-cigarettes (pod system OBY from Aspire© with 1.2 ohm coils) and e-liquids (from Gaiatrend©; menthol and tobacco flavor; nicotine concentrations 3 , 6, and 16 mg/mL; all e-liquids had a ratio of propylene glycol to vegetal glycerin of 70:30), nicotine pouches [from Edelsnus©; menthol (20 mg/g) and mountain herbs (25 mg/g) flavor], and nicotine patches (from Nicotinell©; nicotine concentration 21, 14, and 7 mg/24 h). At inclusion, participants may select one of the offered products. Product changes are permitted at 4 weeks for nicotine patch users and at 8 weeks for users of e-cigarettes or nicotine pouches. At these time points, participants can request supplies or switch products by completing an online questionnaire. In case the questionnaire is not completed, the study team contacts participants by telephone. If participants cannot be reached, the same product as in the previous interval is being provided. At week 16, the study team again contacts participants to organize further supply. However, product changes are no longer possible at this point. In total, participants receive study products free of charge for 24 weeks. All participants receive an information brochure containing usage instructions, potential side effects, and procedures for requesting additional supplies.
Pilot study design and participants
This internal pilot study was prespecified in the RETUNE protocol (Supplementary file Appendix 1). Following the concept of internal pilot studies, all participants included in this report will remain in the trial and be part of the final analysis set11. No formal stopping rules were defined.
We aimed to survey at least 30 intervention participants who accepted one of the offered intervention products. Therefore, we included all participants randomized to the intervention group until we reached these 30 completed interviews for this analysis.
Pilot study data collection and outcomes
We used three different data sources: 1) the linked SHCS data for all characteristics; 2) the trial database that contained the participants’ product choice at baseline; and 3) a pilot study survey via phone call two to four weeks after baseline (Supplementary file Appendix 2).
The SHCS data collection is performed biannually by the treating physician9. All measurements apart from the laboratory measurements are self-reported. We defined alcohol use according to the AUDIT-C (Alcohol Use Disorder Identification Test Consumption) score12. We defined acceptance rate as the proportion of participants who accepted one of the three offered products and signed the respective intervention consent. In this pilot study survey, participants were asked whether they had used the products, about their experiences with the products, and their opinions on the flavor and nicotine concentration. Additionally, participants were queried about the usability of the products and whether they wished to switch to a different product or adjust the flavor or nicotine concentration.
Pilot study statistical analysis
All analyses in the internal pilot study were descriptive. We used medians and interquartile ranges (IQR) for continuous variables and frequencies and percentages for categorical variables. For data management and analysis, we used R, version 4.5.1 (2025-0613; packages used are listed in Supplementary file Appendix 3).
RESULTS
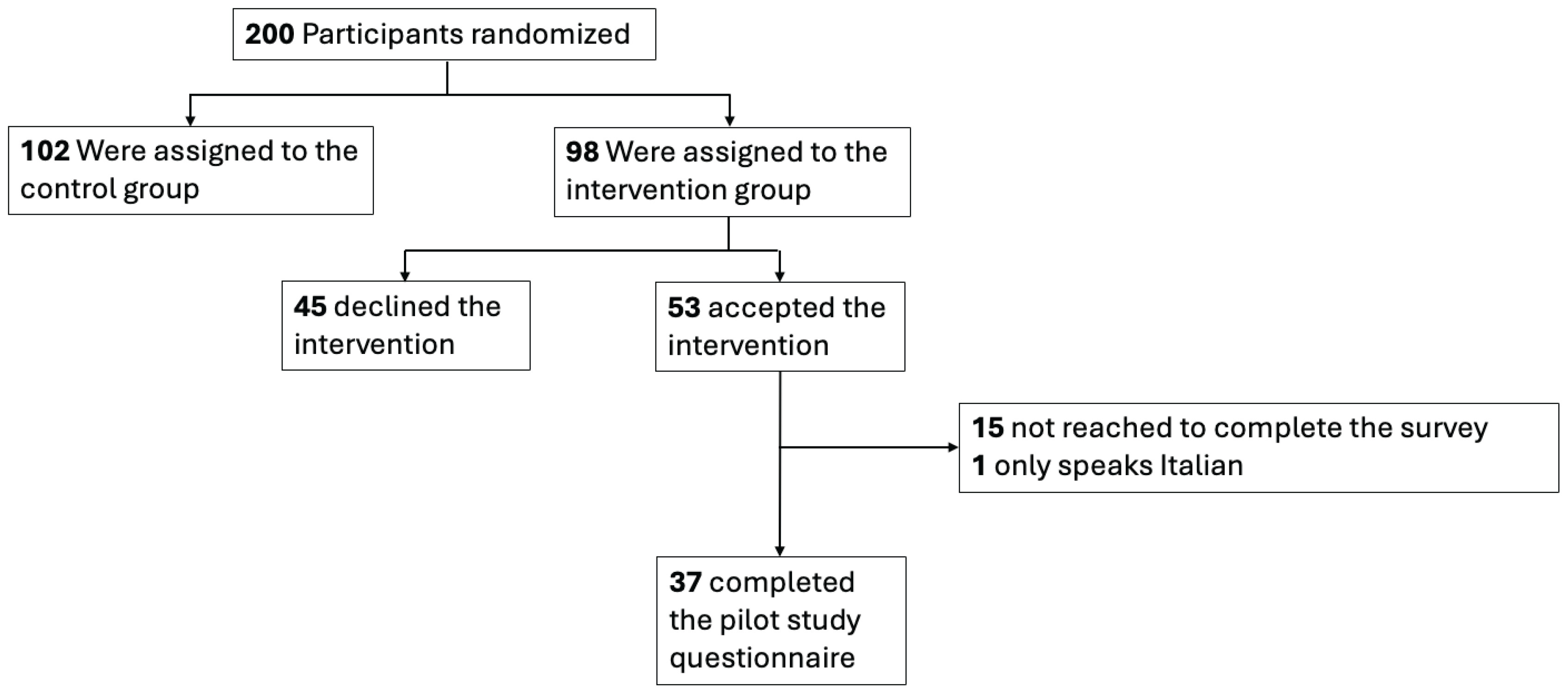
Between 24 February and 3 September 2025, 200 participants were randomized (Figure 1); 98 participants were assigned to the intervention group, and 54.1% of those (53/98) accepted one of the offered nicotine substitute products. Thirty-seven of 53 (69.8%) intervention group participants completed the pilot study survey between 19 March and 2 October 2025.
Figure 1
Flow-chart for the RETUNE internal pilot study. Participants were randomized between February and September 2025 in Switzerland (N=200)
The median age of intervention participants was 57 years (IQR: 43–64) (Table 1). Most participants were male, of European origin, and had no higher education degree. The median number of tobacco cigarettes smoked per day was 13 (IQR: 10–20), and the median number of years of smoking history was 16 (IQR: 10–25). Most participants were adherent to antiretroviral therapy, missing no more than one pill per month, had a viral load below 50 copies/mL, and a median CD4 count of 809 cells/mm3 (IQR: 590–1149). Substance use was common (63/98; 64.3%), mainly Cannabis (47/98; 48.0%), and injectable substance use was rare (3/98; 3.1%). More than one-third (38/98; 38.8%) had excessive alcohol use. There were no obvious numerical differences between participants in terms of acceptance rate, except for substantial variation across sites, ranging from 76.9% (center with the highest acceptance rate) to 9.1% (center with the lowest acceptance rate).
Table 1
Demographic and clinical characteristics of RETUNE pilot study participants (intervention arm only) randomized between February and September 2025 in Switzerland (N=98)
| Characteristics | Overall (N=98) n (%) | Intervention group acceptance (N=53) n (%) | Intervention group refusal (N=45) n (%) |
|---|---|---|---|
| Age (years), median (IQR) | 57 (43–64) | 56 (41–63) | 60 (46–65) |
| Sex (assigned at birth) | |||
| Male | 77 (78.6) | 41 (77.4) | 36 (80.0) |
| Female | 21 (21.4) | 12 (22.6) | 9 (20.0) |
| Higher education degreea,b | 22 (22.4) | 13 (24.5) | 9 (20.0) |
| Origin | |||
| Europe | 85 (86.7) | 47 (88.7) | 38 (84.4) |
| Outside Europe | 13 (13.3) | 6 (11.3) | 7 (15.6) |
| Smoking status | |||
| Cigarettes per day, median (IQR)c | 13 (10–20) | 15 (10–20) | 10 (7–20) |
| Years of tobacco smoking, median (IQR)d | 16 (10–25) | 17 (10–25) | 15 (6–25) |
| Center | |||
| 1 | 40 (40.8) | 27 (50.9) | 13 (28.9) |
| 2 | 13 (13.3) | 10 (18.9) | 3 (6.7) |
| 3 | 2 (2.0) | 0 (0) | 2 (4.4) |
| 4 | 12 (12.2) | 9 (17.0) | 3 (6.7) |
| 5 | 9 (9.2) | 5 (9.4) | 4 (8.9) |
| 6 | 22 (22.4) | 2 (3.8) | 20 (44.4) |
| Missed antiretroviral therapy in the last 4 weeks | |||
| More than once | 8 (8.2) | 2 (3.8) | 6 (13.3) |
| Once | 12 (12.2) | 7 (13.2) | 5 (11.1) |
| Never | 72 (73.5) | 40 (75.5) | 32 (71.1) |
| Not applicable | 6 (6.1) | 4 (7.5) | 2 (4.4) |
| Most likely mode of HIV acquisition | |||
| Men who have sex with men | 45 (45.9) | 25 (47.2) | 20 (44.4) |
| Heterosexual contact | 28 (28.6) | 15 (28.3) | 13 (28.9) |
| People who inject substances | 13 (13.3) | 9 (17.0) | 4 (8.9) |
| Other/unknown | 10 (10.2) | 3 (5.7) | 7 (15.6) |
| Perinatal | 1 (1.0) | 1 (1.9) | 0 (0) |
| Blood products | 1 (1.0) | 0 (0) | 1 (2.2) |
| Viral load (copies/mL) | |||
| <50 | 92 (93.9) | 49 (92.5) | 43 (95.6) |
| 50–399 | 3 (3.1) | 2 (3.8) | 1 (2.2) |
| ≥400 | 3 (3.1) | 2 (3.8) | 1 (2.2) |
| CD4 count (cells/mm³), median (IQR) | 809 (590–1149) | 867 (526–1182) | 763 (628–918) |
| Diagnosis of depressione,f | 8 (8.2) | 7 (13.2) | 1 (2.2) |
| Substance use | |||
| Any substance use | 63 (64.3) | 34 (64.2) | 29 (64.4) |
| Injectable substancesg | 3 (3.1) | 2 (3.8) | 1 (2.2) |
| Cannabish | 47 (48.0) | 26 (49.1) | 21 (46.7) |
| Other substancesi,j | 27 (27.6) | 14 (26.4) | 13 (28.9) |
| In a substance program | 6 (6.1) | 4 (7.5) | 2 (4.4) |
| Excessive alcohol usek | 38 (38.8) | 22 (41.5) | 16 (35.6) |
a Higher education degree: defined as completed higher professional education or university degree above mandatory school (9 years in Switzerland) and finished apprenticeship.
h Frequency cannabis use: daily (n=18), weekly (n=10), monthly (n=8), less frequently (n=9), missing (n=2).
i Other substances: amphetamine/speed, cannabis, cannabidiol (CBD), cocaine, crack cocaine, crystal meth/tina, ecstasy, Gamma-hydroxybutyrate (GHB)/Gamma-butyrilactone (GBL), Ketamine, Lysergic acid.
The most common reason for refusing all offered products was that the participants had no interest in quitting tobacco smoking (34/45; 75.6%) (Table 2). Some participants were not satisfied with the offered products (9/45; 20.0%), others were not willing to participate in a research project (5/45; 11.1%), and one participant (2.2%) was not willing to provide any contact information for supply coordination and therefore declined.
Table 2
Reported reasons of refusal of all the offered products among all participants randomized in the RETUNE intervention arm between February and September 2025 in Switzerland (N=45)
| Reasons for refusal a | n (%) |
|---|---|
| No interest in quitting tobacco smoking | 34 (75.6) |
| Not satisfied by any of the offered products | 9 (20.0) |
| Participant is not willing to participate in a research project | 5 (11.1) |
| Concomitant cannabis use with tobacco | 2 (4.4) |
| Participant is not willing to provide any contact information for supply coordination | 1 (2.2) |
| Participant does not feel supported by any of the products | 1 (2.2) |
| Participant will try quitting without the products and was already in smoking cessations consultation | 1 (2.2) |
| Participant thinks nicotine products are harmful | 1 (2.2) |
| Otherb | 2 (4.4) |
Almost two-thirds of the participants who accepted one of the offered interventions chose e-cigarettes (31/53; 58.5%), one-third chose nicotine patches (17/53, 32.1%), and four participants chose nicotine pouches (4/53; 7.5%) (Table 3). Among the 37 participants who completed the pilot study survey within four weeks after the start of the intervention, most reported that they continued their initially chosen product (27/37; 73.0%), some changed their product (10/37; 27.0%), and nobody stopped using the products (Table 4). The reported side effects were respiratory symptoms (6/28; 21.4%; not asked in patch users), skin reaction (6/37; 16.2%), nausea (3/37; 8.1%), headache (3/37; 8.1%), diarrhea (1/37; 2.7%), constipation (1/37; 2.7%), and mouth irritation (1/28; 3.6%; not asked in patch users); 54.1% (20/37) of the participants did not report any side effects. The side effects by product are provided in Supplementary file Appendix 4.
Table 3
Acceptance of one of the three offered products among all participants randomized in the RETUNE intervention arm between February and September 2025 in Switzerland (N=53)
Table 4
Results of pilot study survey conducted between March and October 2025 in Switzerland (N=37)
| Results | n/N (%) |
|---|---|
| Continued their product without changes during the first 4 weeks follow-up | 27/37 (73.0) |
| Changed/modified product during the first 4 weeks follow-up | 10/37 (27.0) |
| E-cigarettes to nicotine patches | 1/10 (10.0) |
| Nicotine pouches to nicotine patches | 1/10 (10.0) |
| Changed liquid flavor | 2/10 (20.0) |
| Decreased nicotine patch concentration | 1/10 (10.0) |
| Decreased liquid nicotine concentration | 2/10 (20.0) |
| Changed liquid flavor and decreased liquid nicotine concentration | 2/10 (20.0) |
| Increased liquid nicotine concentration | 1/10 (10.0) |
| Stopped the product entirely | 0/37 (0) |
| Adverse event of special interest* | |
| Skin reaction | 6/37 (16.2) |
| Respiratory symptoms (cough, phlegm, wheezing, sore throat)# | 6/28 (21.4) |
| Nausea | 3/37 (8.1) |
| Headache | 3/37 (8.1) |
| Mouth irritation# | 1/28 (3.6) |
| Diarrhea | 1/37 (2.7) |
| Constipation | 1/37 (2.7) |
| Emesis | 0/37 (0) |
| Dizziness | 0/37 (0) |
| Mouth ulcers# | 0/28 (0) |
| Gingival pain# | 0/28 (0) |
| Gingival bleeding# | 0/28 (0) |
| No adverse events of special interest | 20/37 (54.0) |
* Several answer options per participant possible; stratified table by product provided in Supplementary file Appendix 4.
The experiences of 24 e-cigarette users are summarized in Supplementary file Appendix 5, where 65% (15/23) rated their experience overall as positive, and 35% (8/23) as neutral; 54% (13/24) of participants liked the flavor of the chosen liquids, while 33% (8/24) were neutral, and 26% (6/23) wished to change to another flavor when asked during the survey; 59% (13/22) of the participants rated the nicotine concentration of the liquids as ‘just right’, while 41% (9/22) rated the concentration as ‘too high’ or ‘too low’. Most participants perceived the e-cigarette as easy to handle (76%; 16/21) and useful to quit tobacco smoking (59%; 13/22). Among the 9 participants who used nicotine patches and filled in the survey, 75% (6/8) had an overall positive impression (Supplementary file Appendix 6); 56% (5/9) rated the nicotine concentration of the patches as ‘just right’, while 44% (4/9) rated the concentration as ‘too high’ or ‘too low’. All participants perceived the patches as easy to handle, and 75% (6/8) thought they were useful to quit tobacco smoking.
Among the four participants who chose nicotine pouches, two rated the flavor and the overall experience with the pouches as positive, and two as neutral (Supplementary file Appendix 7). No participant wanted another flavor, and all rated the nicotine concentration as ‘just right’. Two of the participants stated they had received enough information on the product, three believed that the pouches are useful to quit tobacco smoking, while one participant was neutral.
DISCUSSION
This internal pilot study included the first 98 participants randomized to the intervention arm. The acceptance rate of one of the interventions was 54%, which is similar to our estimated 50%. E-cigarettes were the most popular product of the offered menu, followed by nicotine patches. In the subsample of surveyed intervention participants, all products (e-cigarettes, nicotine patches, nicotine pouches) were mostly rated positively. Most participants continued using the same product they had initially chosen (i.e. including the same flavor and nicotine strength) beyond the 4-week pilot phase, and no one stopped the cessation intervention altogether.
The proposed mechanism of action of the RETUNE trial is that participants will not only accept the offered products but also use them. This pilot study showed high engagement from the participants, which supports this proposed mechanism. Similarly, high engagement was observed by Carpenter et al.13 in a large smoking-cessation trial in the United States that offered e-cigarettes and also used an ‘opt-out’ approach, i.e. offering to participants irrespective of willingness to quit smoking. In a Swiss observational study, Auer et al.14 showed high uptake of smoking cessation counselling when offered to all smokers hospitalized with acute coronary syndrome in an ‘opt-out’ approach. The TwiCs design allowed us to implement such an opt-out approach in an efficient and fully embedded way in a running cohort study. Existing literature suggests that motivation to quit smoking is often overemphasized and may create barriers to accessing cessation support and participation in smoking cessation trials15,16. In comparison with a previous traditional ‘opt-in’ smoking cessation trial conducted in the SHCS17, our study achieved higher participation rates. However, direct attribution of this improvement to the trial design is challenging given the use of different interventions in the two trials. Notably, among the pilot study participants, smoking patterns were similar between participants who accepted and those who refused the intervention. This finding supports the concept that commonly used indicators, such as the number of cigarettes smoked per day, are unreliable predictors of an individual’s willingness to engage in smoking-cessation efforts18,19. Unsurprisingly, the most common reason for refusing all products was no interest in quitting tobacco smoking. Only two participants explicitly declined the offered intervention due to cannabis use, despite the common use of cannabis (48%) in the intervention group. If the RETUNE intervention also influences cannabis use or if ongoing cannabis use might interfere with the tobacco abstinence outcome, it remains to be investigated.
In trials using the TwiCs design, the acceptance rate of the offered intervention is a key aspect7. High refusal rates dilute the intention-to-treat estimate. Therefore, refusal should be anticipated and considered when calculating the trial sample size20. We calculated the sample size based on an anticipated acceptance of 50% and will continue recruitment after these reassuring results from the pilot study. Following the protocol, we will continuously reevaluate the acceptance rate. However, the pilot results show substantial differences in the acceptance rate across centers. These differences were unexpected, especially because there are no notable differences in participant characteristics, and the trial implementation process was comparable across centers. Further research is planned to investigate the reasons for varying acceptance rates across centers.
A further goal of the pilot study was to adapt the menu of offered products based on early participant feedback. E-cigarettes were the most popular product. However, only 60% of users were satisfied with the nicotine strength they had chosen. Therefore, we expanded the menu with two additional nicotine concentrations (0 mg/mL and 12 mg/mL). This change is reflected in the newest protocol version 1.2. Nicotine patches were the second most popular product and were also rated positively regarding handling and their perceived support for quitting tobacco smoking. The main issue was again nicotine dosing. Because patches are commercially available only in fixed strengths and are usually used in step-down regimens, we could not adjust the dosing of this product. Nicotine pouches were the least popular option. This may be explained by the average age of the study population, as nicotine pouches tend to be more common among younger people21. Moreover, participants without prior experience in using nicotine pouches may not have found them an appealing product.
To date, no randomized trial has offered e-cigarettes, nicotine patches, and nicotine pouches as a preference-based menu to tobacco smokers. Our findings on product popularity align with recent population-based data from England, where about 40% of smokers with a recent quit attempt used e-cigarettes, about 17% used over-the-counter nicotine replacement therapy including patches, and about 3% used nicotine pouches22. Results from a French pilot study among smokers with low socioeconomic status showed similar results for e-cigarettes and nicotine replacement therapy23.
Limitations
Our study has the following limitations. First, we could not reach all participants within the first four weeks after randomization to complete the pilot study questionnaire (response rate: 70%). Therefore, it is possible that participants with negative experiences or generally lower motivation to provide data were underrepresented. This may have led to an overestimation of the positive perceptions of the intervention products and an underestimation of early discontinuation rates within the first four weeks. Second, the surveys were conducted by the study team via telephone, which may have influenced how participants responded to the questions, i.e. we cannot exclude social desirability bias. However, the real-time follow-up minimized recall-bias and helped to directly improve the implementation process. Third, the use of self-reported SHCS data could result in data misclassification, e.g. of smoking behavior, drug adherence, mode of HIV acquisition, depression, alcohol use, and substance use. Fourth, only four people chose the nicotine pouches which makes it difficult to assess experiences and side effects with this product. Fifth, the additional contact for the pilot study survey could potentially influence the intervention effectiveness. We plan to perform a corresponding sensitivity analysis in the effectiveness analysis to investigate this hypothesis.
CONCLUSIONS
The results of this internal pilot support the feasibility of the RETUNE trial. The observed acceptance rate was similar to our estimated acceptance rate. E-cigarettes were the preferred product and satisfaction with all products was high. With minor changes to the intervention menu, we are continuing participant recruitment.