
INTRODUCTION
Tobacco susceptibility – the absence of a firm commitment not to smoke in the future – is among the strongest predictors of subsequent smoking initiation in never smoking youth and young adults1,2. While aggregate susceptibility prevalence provides useful population-level data, it may mask meaningful heterogeneity. In contexts where both cigarettes and e-cigarettes are widely available, susceptibility patterns may differ across individuals: some may be susceptible primarily to one product, others to both, and some may hold uncertain rather than definitive attitudes. Identifying these distinct profiles and their associated characteristics could inform more appropriately targeted prevention strategies2.
Latent class analysis (LCA) is a person-centered statistical method that identifies unobserved subgroups based on shared response patterns across categorical indicators3. LCA has been applied to characterize tobacco use patterns in several populations, including polytobacco use profiles among US college students4 and adult tobacco product use frequencies5. Separately, Cheng et al.21 examined whether youth susceptibility to multiple tobacco products reflects a general or product-specific construct, finding that a general susceptibility factor dominated the prediction of initiation. In the Chinese context, however, LCA has been less commonly applied to tobacco susceptibility research, and the question of whether distinct susceptibility subgroups exist among Chinese college students who have never used tobacco remains largely unexplored.
China’s tobacco landscape creates a relevant context for this question. The 2021 national survey reported a 7.8% current smoking rate among college students6, while e-cigarette awareness exceeds 94%, with ever use rates of 4–16%7,8. A recent study among Chinese college students identified bar attendance, alcohol consumption and exposure to e-cigarette marketing as the strongest behavioral predictors of e-cigarette use susceptibility22. Furthermore, a cross-national survey including China reported that 82% of Chinese young people who had never used e-cigarettes expressed some degree of susceptibility, the highest rate among the four countries studied23. These findings suggest that e-cigarette susceptibility among Chinese young adults may be particularly prevalent and warrants closer examination. The policy environment further shapes these dynamics: provinces with comprehensive smoke-free legislation benefit from tobacco denormalization, while provinces without such legislation – including the present study setting, which lacks a comprehensive smoke-free law – may harbor distinct susceptibility patterns in which individual-level risk factors carry proportionally greater weight9.
This study aimed to: 1) describe the prevalence and item-level patterns of cigarette and e-cigarette susceptibility among tobacco-naïve Chinese college students, including the degree of concordance between the two products; 2) identify latent classes of susceptibility using six dual-product indicators; and 3) characterize the identified classes by demographic, psychological, and behavioral profiles.
METHODS
Study design and participants
A cross-sectional survey was conducted in December 2025 among undergraduate students at a public university in Fujian Province, southeastern China. This institution is a teacher-training university with an enrollment composition of approximately 75% female students, which is reflected in the sample. Eligible participants were full-time enrolled undergraduates aged ≥18 years across the four academic years (freshman to senior) who provided written informed consent. Stratified random sampling across four academic years was used. Of 492 distributed online questionnaires, 415 valid responses were retained after excluding completion times <3 minutes and non-undergraduate respondents (response rate: 84.35%). The analytic sample for the present latent class analysis comprised 368 students who reported never having used either cigarettes or e-cigarettes, even one or two puffs (i.e. the tobacco-naïve subsample). The study was approved by the Research Ethics Committee of Fujian Polytechnic Normal University (Approval No. 2025-07), and all participants provided informed consent. Reporting followed the STROBE guidelines13.
Measures
Tobacco use and susceptibility
Tobacco use was assessed by asking whether participants had ever tried cigarettes or e-cigarettes, even one or two puffs. Tobacco susceptibility was measured using the validated Pierce algorithm1, adapted for both cigarettes and e-cigarettes. Three items assessed cigarette susceptibility (‘Do you think you will try smoking a cigarette in the next 12 months?’; ‘If one of your best friends offered you a cigarette, would you smoke it?’, ‘At any time in the future, do you think you will smoke a cigarette?’) and three parallel items assessed e-cigarette susceptibility. Response options were ‘definitely not’, ‘probably not’, ‘probably yes’, and ‘definitely yes’. For LCA, each item was dichotomized as 0 (‘definitely not’) versus 1 (any other response), consistent with the standard Pierce algorithm operationalization1,2. This dichotomization was chosen because the theoretical construct of susceptibility is defined by the absence of a firm commitment to abstain; the distinction between ‘probably not’ and ‘probably yes’ is secondary to the presence or absence of firm refusal. The full four-level response distributions are presented to enable the reader’s evaluation of potential information loss.
Tobacco health knowledge and e-cigarette cognition
Tobacco health knowledge was measured using four items referencing the GATS core questionnaire14, asking whether smoking causes stroke, heart disease, lung cancer and erectile dysfunction (correct answer: ‘yes’; total score 0–4). E-cigarette awareness was assessed with a single item: ‘Have you heard of e-cigarettes?’ (yes, no). E-cigarette cognition was assessed through two items rated on a 5-point Likert scale (1=strongly disagree to 5=strongly agree): ‘Using e-cigarettes is addictive’ and ‘Once you start using e-cigarettes, it is difficult to quit’. An additional item assessed perceived social image: ‘Using e-cigarettes makes people look more attractive’ (same 5-point scale).
Psychological measures
Depressive symptoms were measured with the 10-item Center for Epidemiologic Studies Depression Scale (CES-D-10)15 score 0–30 with ≥10 indicating clinically significant symptoms. The Chinese version has been validated in college student populations with demonstrated adequate psychometric properties15. Psychological resilience was measured with the 6-item Brief Resilience Scale (BRS)16, mean score 1–5. The Chinese version has been used in prior studies of young adult populations16. Sample-specific reliability indices for both scales are reported in the Results section. Social support was assessed using a 5-item scale measuring perceived adaptability, problem-solving capacity, friend support, family support and confidant availability (total score 5–25).
Covariates were defined as follows: sex (male, female), academic year (freshman, sophomore, junior, senior), household registration (urban, rural), monthly expenditure (RMB) (≤1500, 1501–2500, >2500), parental smoking status (any biological parent currently smokes: yes, no), close friends’ smoking status (any close friend currently smokes: yes, no), and alcohol consumption (any alcohol use in the past 30 days: yes, no). Based on prior literature linking these characteristics with adolescent and young-adult tobacco susceptibility, sex, household registration, parental smoking, peer smoking, and alcohol consumption were specified a priori as potential confounders for class–covariate associations.
Statistical analysis
Descriptive statistics summarized sample characteristics and item-level susceptibility distributions. Concordance between cigarette and e-cigarette susceptibility was assessed using Cohen’s kappa (κ) and the phi (φ) coefficient. Latent class models with 2 to 5 classes were estimated using the Expectation–Maximization (EM) algorithm with 100 random starting values per model to ensure convergence to the global maximum3. Model selection was guided by the Bayesian Information Criterion (BIC; lower preferred), Akaike Information Criterion (AIC), classification entropy (≥0.80 indicates adequate classification)3 and substantive interpretability. Models producing classes containing fewer than 5% of the sample were considered with caution due to potential instability. Formal likelihood ratio difference tests (LMR-LRT, BLRT) were not available in the present implementation; this limitation is addressed by the convergent evidence from BIC, entropy and interpretability.
Following class enumeration, identified classes were characterized by comparing covariates using one-way ANOVA with F-statistics and degrees of freedom for continuous variables, and Pearson chi-squared tests with degrees of freedom for categorical variables. Post hoc pairwise comparisons used Tukey’s honestly significant difference (HSD) procedure for continuous variables (controlling the family-wise error rate at 0.05) and Wald-based 95% confidence intervals for prevalence differences for categorical variables. For continuous variables, mean differences with 95% confidence intervals (CIs) and partial η2 are reported as effect-size estimates; for categorical variables, prevalence differences with 95% CIs are reported. Analyses were conducted in Python (SciPy 1.12, NumPy 1.26) with a custom EM implementation verified against the poLCA package in R 4.3, confirming identical class assignments and comparable fit indices. Statistical significance was set at p<0.05 (two-tailed).
RESULTS
Sample characteristics
The analytic sample comprised 368 tobacco-naïve students (79.3% female, mean age=21 years). The sex ratio is consistent with the enrolment composition of the study institution, a teacher-training university. Demographic, behavioral and psychological characteristics are presented in Table 1. Nearly half of participants (48.6%) met the threshold for clinically significant depressive symptoms (CES-D-10 ≥10). The mean tobacco health knowledge score was 2.92 ± 1.39 out of 4, with the highest awareness for lung cancer (91.3%) and the lowest for heart disease (63.6%). Regarding e-cigarettes, 94.6% had heard of e-cigarettes, 84.5% agreed or strongly agreed that e-cigarette use is addictive, and 82.1% agreed or strongly agreed that e-cigarettes are difficult to quit once started. Over half (54.3%) reported having close friends who smoke, and 35.6% reported alcohol consumption.
Table 1
Characteristics of the analytic sample of tobacco-naïve undergraduate students, a cross-sectional survey at a public university in Fujian Province, China, December 2025 (N=368)
| Characteristics | n (%) |
|---|---|
| Sex | |
| Male | 76 (20.7) |
| Female | 292 (79.3) |
| Academic year | |
| Freshman | 144 (39.1) |
| Sophomore | 58 (15.8) |
| Junior | 128 (34.8) |
| Senior | 38 (10.3) |
| Household residence | |
| Urban | 201 (54.6) |
| Rural | 167 (45.4) |
| Monthly expenditure (RMB) | |
| ≤1500 | 126 (34.2) |
| 1501–2500 | 214 (58.2) |
| >2500 | 28 (7.6) |
| Social and behavioral factors | |
| Parent smokes | 198 (53.8) |
| Close friends smoke | 200 (54.3) |
| Alcohol consumption (past 30 days) | 131 (35.6) |
| Tobacco and e-cigarette cognition | |
| E-cigarette awareness | 348 (94.6) |
| E-cigarettes are addictive (agree/strongly agree)* | 311 (84.5) |
| E-cigarettes are difficult to quit (agree/strongly agree) | 302 (82.1) |
| Tobacco knowledge score (0–4), mean ± SD | 2.92 ± 1.39 |
| Tobacco harm correct knowledge | |
| Lung cancer | 336 (91.3) |
| Erectile dysfunction | 256 (69.6) |
| Stroke | 248 (67.4) |
| Heart disease | 234 (63.6) |
| Secondhand smoke (SHS) harm awareness | 318 (86.4) |
| Psychological measures | |
| CES-D-10 score (Cronbach’s α=0.879), mean ± SD | 9.64 ± 5.96 |
| Clinically significant (≥10) | 179 (48.6) |
| BRS score (Cronbach’s α=0.537), mean ± SD | 3.34 ± 0.59 |
| Social support score (Cronbach’s α=0.941), mean ± SD | 18.83 ± 4.37 |
Reliability of psychological measures in the analytic sample
Internal consistency was acceptable for the CES-D-10 (Cronbach’s α=0.879) and the social support scale (α=0.941), but low for the BRS (α=0.537). Item-deletion analysis indicated that no single BRS item removal would improve reliability (all Δα negative). Inter-item correlations among BRS items showed a pattern consistent with a method factor associated with reverse-scored items (positive–positive r=0.62 to 0.75; negative–negative r=0.62 to 0.75; cross-valence r= -0.14 to -0.24). Accordingly, BRS-based findings are reported descriptively and interpreted with caution in the Discussion.
Cigarette and e-cigarette susceptibility
Item-level response distributions are presented in Table 2. Across all six items, ‘definitely not’ was the predominant response (87.8–90.5%). Among those expressing any degree of susceptibility, ‘probably not’ was most common (4.9–7.1%), followed by ‘probably yes’ (2.7–4.1%) and ‘definitely yes’ (1.1%). Future-oriented items received the highest susceptibility endorsement for both cigarettes (12.2%) and e-cigarettes (11.7%), while 12-month intention items had the lowest (both 9.5%).
Table 2
Cigarette and e-cigarette susceptibility among tobacco-naïve undergraduate students, a cross-sectional survey at a public university in Fujian Province, China, December 2025 (N=368)
Overall, 56 participants (15.2%) were susceptible to at least one tobacco product: 50 (13.6%) to cigarettes, 48 (13.0%) to e-cigarettes, and 42 (11.4%) to both simultaneously (Table 2). Product-specific susceptibility was uncommon: only 8 students (2.2%) were susceptible to cigarettes alone, and 6 (1.6%) to e-cigarettes alone. The concordance between cigarette and e-cigarette susceptibility was high (Cohen’s κ=0.835; φ=0.835, p<0.001). Males exhibited higher susceptibility than females for both cigarettes (23.7% vs 11.0%) and e-cigarettes (21.1% vs 11.0%).
Latent class model selection
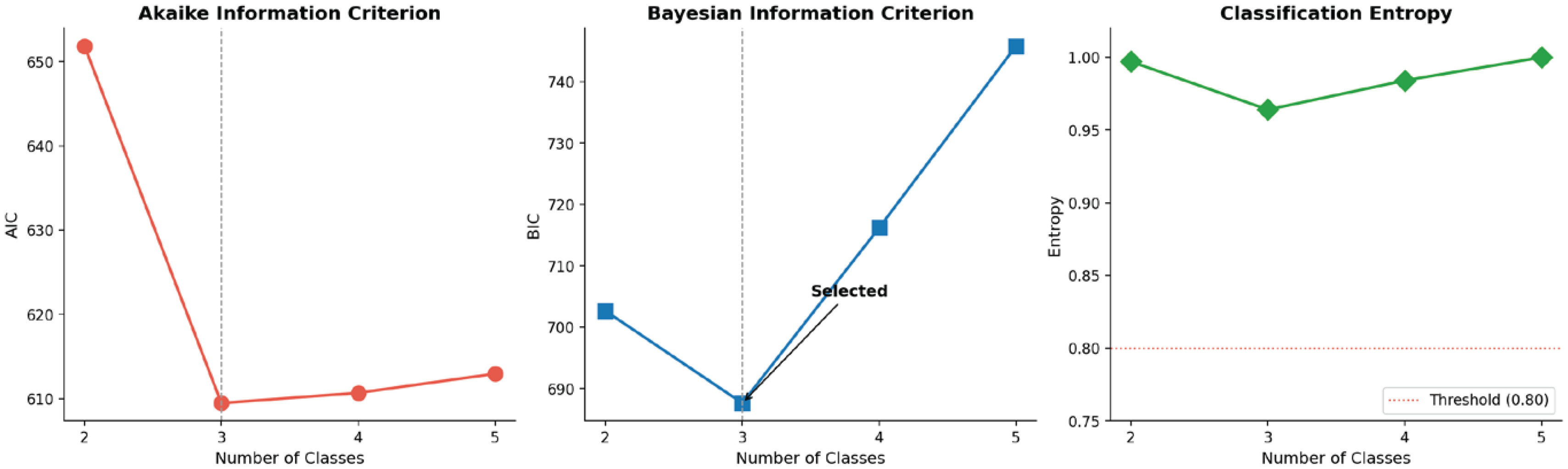
Model fit indices for 2- to 5-class solutions are presented in Table 3 and Figure 1. The 3-class model yielded the lowest BIC (687.85), with BIC increasing for the 4- and 5-class solutions (718.04 and 753.80, respectively). AIC continued to decrease slightly from 3 to 4 classes, but the improvement was marginal (609.69 vs 612.52). All solutions achieved entropy >0.96, indicating excellent classification quality. The 4-class solution produced a class of only 1.1% (n=4), and the 5-class solution a class of 0.8% (n=3), raising concerns about stability and replicability. All models converged consistently across 100 random starting values. The 3-class solution was selected based on the lowest BIC, the smallest class size (5.4%, n=20) and substantive interpretability.
Table 3
Model fit indices for 2- to 5-class latent class analysis solutions of cigarette and e-cigarette susceptibility among tobacco-naïve undergraduate students, a cross-sectional survey at a public university in Fujian Province, China, December 2025 (N=368)
| Classes | LL | Parameters | AIC | BIC | Entropy | Smallest class |
|---|---|---|---|---|---|---|
| 2 | -312.92 | 13 | 651.84 | 702.64 | 0.997 | 10.3% (N=38) |
| 3* | -284.73 | 20 | 609.46 | 687.62 | 0.964 | 5.4% (N=20) |
| 4 | -278.34 | 27 | 610.68 | 716.20 | 0.984 | 1.1% (N=4) |
| 5 | -272.47 | 34 | 612.94 | 745.81 | 1.000 | 0.8% (N=3) |
LL: log-likelihood. AIC: Akaike Information Criterion; BIC: Bayesian Information Criterion; lower BIC is preferred. Entropy ≥0.80 indicates adequate classification.
* Selected model. Models were estimated using the Expectation–Maximization algorithm with 100 random starting values; all models converged consistently. Values reflect the verified replication on the original cleaned dataset. Differences from a previous internal report (BIC=687.85) are within EM convergence precision and do not change the selected model or any class assignment.
Three-class solution
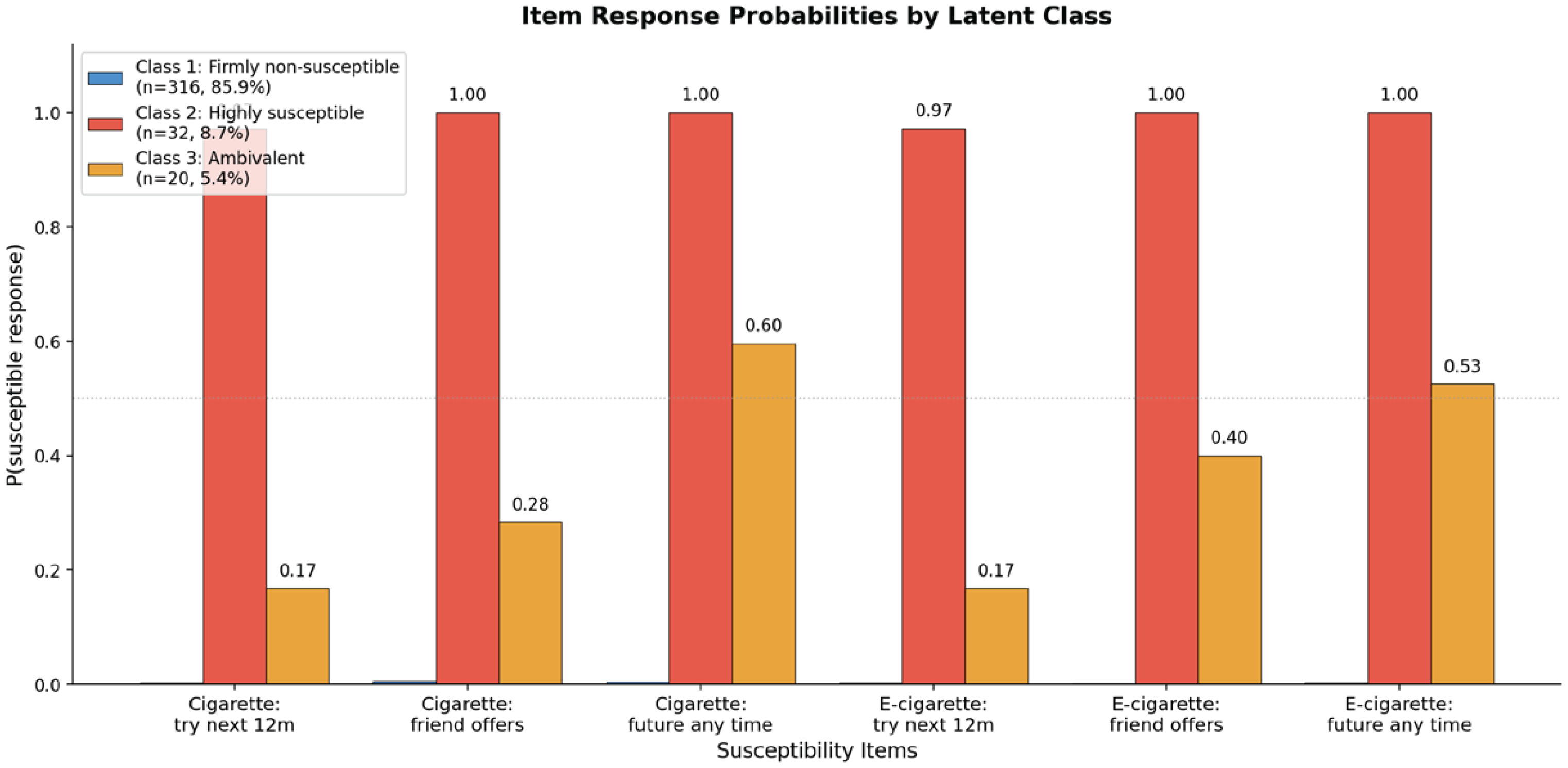
Item response probabilities for the 3-class solution are presented in Table 4 and Figure 2. Class 1, labeled ‘firmly non-susceptible’, comprised 85.9% of the sample (n=316) and was characterized by near-zero probability of endorsing any susceptibility item (all <0.01). Class 2, labeled ‘highly susceptible’, comprised 8.7% (n=32) and exhibited near-universal endorsement across all six items (probabilities 0.97–1.00), indicating strong susceptibility to both cigarettes and e-cigarettes without product differentiation. Class 3, labeled ‘ambivalent’, comprised 5.4% (n=20) and displayed a selective pattern: moderate endorsement of future-oriented items (cigarette 0.60; e-cigarette 0.53) coupled with lower endorsement of 12-month intention items (both 0.17) and peer-offer items (cigarette 0.29; e-cigarette 0.40).
Table 4
Item response probabilities by latent class (3-class solution) of cigarette and e-cigarette susceptibility among tobacco-naïve undergraduate students, a cross-sectional survey at a public university in Fujian Province, China, December 2025 (N=368)
Class characterization
Demographic, psychological, and behavioral profiles are presented in Table 5 and Figure 3. Compared with Class 1, Class 2 had significantly lower tobacco health knowledge [1.69 ± 1.67 vs 3.06 ± 1.30; MD= -1.38; 95% CI: -1.96 – -0.79; partial η2=0.081; F(2, 365)=16.03; p<0.001; Tukey HSD-adjusted pairwise p<0.001] and higher CES-D-10 scores [12.88 ± 6.66 vs 9.25 ± 5.88; MD=3.62; 95% CI: 1.05–6.19; partial η2=0.031; F(2, 365)=5.75; p=0.004; Tukey HSD-adjusted pairwise p=0.003]. Class 2 included a higher proportion of male students [40.6% vs 18.7%; prevalence difference 22.0 percentage points, 95% CI: 4.4–39.5; χ2(2)=8.55, p=0.014], students with smoking friends [81.2% vs 50.6%; prevalence difference 30.6 percentage points, 95% CI: 16.0–45.2; χ2(2)=13.07; p=0.002], students who consume alcohol [59.4% vs 32.0%; prevalence difference 27.4 percentage points, 95% CI: 9.6–45.2; χ2(2)=13.00; p=0.002], and students with urban household registration [75.0% vs 51.9%; prevalence difference 23.1 percentage points, 95% CI: 7.1–39.1; χ2(2)=7.18; p=0.028].
Table 5
Class characterization by demographic, psychological, and behavioral variables among tobacco-naïve undergraduate students, a cross-sectional survey at a public university in Fujian Province, China, December 2025 (N=368)
[i] For continuous variables, the effect size column reports partial η² for the overall ANOVA, and the rightmost column reports the Tukey HSD-adjusted mean difference (MD) with 95% CI for Class 2 vs Class 1. For categorical variables, the effect size is Cramér’s φc, and the rightmost column reports the prevalence difference (Δp, in percentage points) with 95% Wald CI for Class 2 vs Class 1. CES-D-10: 10-item Center for Epidemiologic Studies Depression Scale. BRS: Brief Resilience Scale. MD: mean difference. pp: percentage points. HSD: honestly significant difference. Tukey HSD-adjusted post hoc p-values for the principal Class 1 vs Class 2 contrasts: CES-D-10 p=0.003; tobacco knowledge p<0.001. BRS-related findings should be interpreted with caution because of low internal consistency in the present sample (Cronbach’s α=0.537).
Figure 3
Psychological and behavioral profiles by latent class among tobacco-naïve undergraduate students, a cross-sectional survey at a public university in Fujian Province, China, December 2025 (N=368)
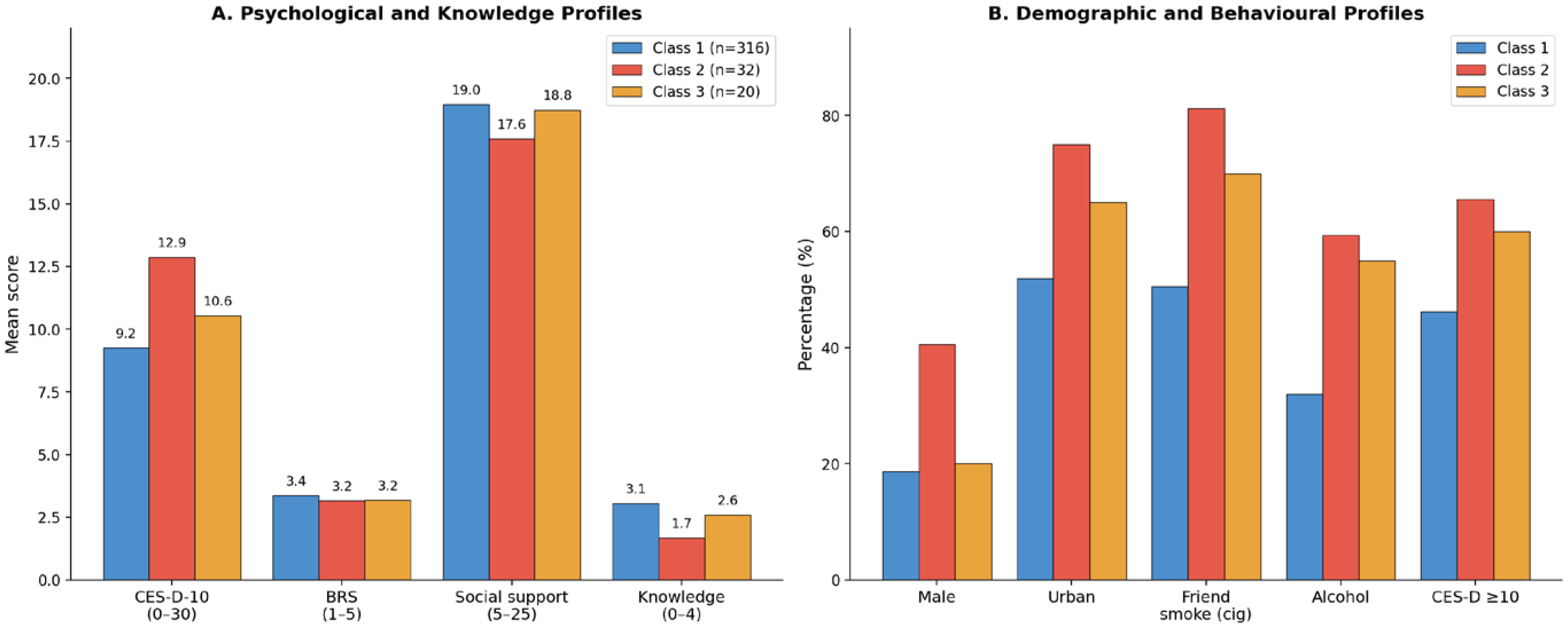
Class 3 occupied an intermediate position on most variables. Knowledge scores were numerically but not statistically lower than Class 1 after Bonferroni correction (2.60 vs 3.06; corrected p=0.369), which may reflect limited statistical power given the small class size (n=20). BRS resilience scores did not differ significantly across classes [F(2, 365)=2.42; p=0.090]. Social support [F(2, 365)=1.42; p=0.243] and parental smoking [χ2(2)=2.03; p=0.362] also did not differ across classes.
DISCUSSION
This cross-sectional study yielded three principal findings. First, three distinct latent classes of tobacco susceptibility were identified among tobacco-naïve Chinese college students: a firmly non-susceptible majority, a small highly susceptible class, and a smaller ambivalent class. Second, susceptibility showed high concordance between cigarettes and e-cigarettes, with product-specific susceptibility being uncommon. Third, the highly susceptible class was characterized by a convergent profile of lower tobacco health knowledge, higher depressive symptoms, peer smoking exposure, and alcohol use, while the ambivalent class showed selective endorsement of distal future-oriented items but not of imminent-intention items. To our knowledge, this is one of the first applications of latent class analysis to dual-product tobacco susceptibility in a Chinese young-adult population, offering a person-centered perspective that extends beyond the binary susceptible/non-susceptible classification commonly used in prior research.
The high concordance between cigarette and e-cigarette susceptibility, combined with the rarity of product-specific susceptibility, suggests that susceptibility in this sample operated largely as a generalized disposition. This finding is consistent with Cheng et al.21 who demonstrated, using Population Assessment of Tobacco and Health (PATH) Study data, that a general susceptibility factor dominated the prediction of tobacco initiation among US youth. It also aligns with the cross-national evidence from Pettigrew et al.23 who found that conventional tobacco use was a significant predictor of e-cigarette susceptibility across four countries, including China, suggesting shared underlying vulnerability. This observation has potential methodological implications: in populations where both products are widely known, studies measuring only cigarette susceptibility may capture most e-cigarette-susceptible individuals as well. However, this pattern may be context-dependent. In populations where e-cigarettes are perceived as fundamentally different from cigarettes – for example, due to targeted marketing or different regulatory environments – greater product specificity in susceptibility might be expected20. Future research should examine whether this concordance holds across diverse Chinese university populations.
The three identified classes warrant separate consideration in future research. The firmly non-susceptible majority represents students with consolidated anti-tobacco attitudes for whom existing environmental protective factors, such as campus smoke-free policies, may be sufficient. The highly susceptible class exhibits a convergent risk profile – lower health knowledge, higher depressive symptoms, male sex, peer smoking exposure, and alcohol use – that identifies measurable, candidate criteria for future screening and targeted intervention research. The knowledge deficit is particularly notable: the highly susceptible class identified substantially fewer smoking-caused diseases on average than the firmly non-susceptible class, and overall sample awareness of stroke and heart disease as smoking-related outcomes was relatively low. Health education addressing specific disease outcomes, particularly stroke and heart disease, represents a candidate, potentially modifiable target that warrants prospective evaluation.
Chen et al.24 further demonstrated that protection motivation cognitions – particularly perceived severity and self-efficacy – significantly predicted e-cigarette susceptibility among Chinese college students, supporting the potential of theory-based educational interventions. Importantly, because susceptibility was associated with both cigarette and e-cigarette products, educational research that addresses one product type could in the future be evaluated for whether it also affects susceptibility to the other.
The ambivalent class endorsed future-oriented susceptibility items at moderate probability but not items reflecting immediate intention, suggesting cognitive uncertainty rather than active planning. The distinct profile of this group, relative to the highly susceptible class, supports the value of person-centered approaches over binary susceptibility classifications2 and motivates future studies to assess whether universal-level approaches, such as smoke-free policies and social-norm interventions17, might be especially relevant for this subgroup.
The co-occurrence of alcohol consumption with tobacco susceptibility in the highly susceptible class is consistent with evidence of health-risk-behavior clustering among young adults18 and provides a candidate target for integrated future research on multi-behavior interventions. Mean depressive symptoms in the highly susceptible class exceeded the conventional clinical threshold21-23, raising the question – to be addressed by future longitudinal work – of whether linking tobacco-prevention research with campus mental-health services would be informative; the present cross-sectional design cannot determine whether depressive symptoms precede, follow, or co-occur with susceptibility cognitions.
Strengths and limitations
Strengths of the study include the validated Pierce algorithm adapted for dual-product susceptibility, the detailed item-level susceptibility data enabling concordance analysis and the broad covariate set.
Several limitations should be acknowledged. First, the cross-sectional design precludes causal inference; associations between class membership and covariates should be interpreted as non-causal. Second, the sample is from a single teacher-training university with approximately 75% female enrolment, which is reflected in the analytic sample (79.3% female). This sex ratio limits the generalizability of findings to male students and to institutions with different enrolment compositions (e.g. engineering or science universities with predominantly male enrolment). The substantially higher susceptibility among males (relative to females) suggests that studies with more balanced sex ratios might identify different class structures. Third, the EM algorithm implementation does not yield formal likelihood ratio tests (LMR-LRT, BLRT); however, convergent evidence from BIC (lowest for the 3-class solution), high entropy, consistent convergence across 100 random starts, and substantive interpretability support the selected solution. Fourth, the small sizes of the highly susceptible and ambivalent classes constrain statistical power for detecting between-class differences, particularly for the ambivalent class. Fifth, the low BRS internal consistency limits interpretation of resilience findings; item-deletion analysis confirmed that no individual item removal would improve reliability, and the pattern of inter-item correlations was consistent with a method factor associated with reverse-scored items. Future studies should consider alternative resilience measures with stronger psychometric properties in Chinese populations, such as the Connor-Davidson Resilience Scale19. Sixth, the dichotomization of susceptibility indicators may result in some information loss; however, the high correlation between ordinal and binary item sums (r=0.914) suggests that the classification would be largely consistent under alternative coding schemes. Seventh, residual confounding from unmeasured variables – including parental education, family socioeconomic status, prior psychiatric history, and exposure to e-cigarette marketing – cannot be ruled out and may explain part of the observed class–covariate associations. Eighth, the data are entirely self-reported, which may introduce information bias and outcome misclassification, particularly for sensitive items such as alcohol use, depressive symptoms and tobacco-related cognitions; the direction of any such bias cannot be predicted a priori.
CONCLUSIONS
Three distinct tobacco susceptibility profiles were identified among tobacco-naïve Chinese college students at a single institution in southeastern China: a firmly non-susceptible majority, a highly susceptible class characterized by lower health knowledge, higher depressive symptoms, peer smoking exposure, and alcohol use and an ambivalent class with selective future-oriented uncertainty. The high concordance between cigarette and e-cigarette susceptibility suggests that, in this sample, susceptibility operated largely as a generalized tobacco disposition. These findings are hypothesis-generating and require confirmation in multi-site longitudinal studies with more balanced sex representation before they can inform differentiated tobacco-prevention practice.