

INTRODUCTION
Secondhand smoke and aerosol in California
In spite of on-going attempts to limit outdoor exposures to secondhand smoke (SHS) and aerosol (SHA) in California through statewide and municipal ordinances, the California Youth Tobacco Survey 2024 found that >60% of high school students were exposed to SHS or SHA in the past two weeks in an outdoor location, with a higher percentage of Latino adolescents exposed compared with Asians, African-Americans and those that identified as Other1. Exposure to SHS and SHA may be particularly concerning for Latinos in California as 44% live in areas with poor air quality compared with 25% of other ethnic and racial groups2. Additionally, Latino children under 10 years of age make up 81% of those living in the most polluted areas.
Senate Bill (SB) 793
In efforts to reduce the burden of chronic disease related to tobacco use, California has made attempts to decrease the overall tobacco product use and initiation, particularly among adolescents. California voters passed Senate Bill (SB) 793 in 2022, which prohibits the sale of flavored tobacco products in California. This law went into effect on 1 January 20233. In 2024, electronic nicotine delivery systems (ENDS), including e-cigarette product use, remained the most commonly used tobacco product type for US adolescents4.
SB 793 has the potential to dramatically reduce ENDS product use among Californian adolescents. Previous studies have suggested that youth prefer flavored products with 79.1% of US adolescent users reporting flavored consumption5. Meanwhile, a study conducted pre- and post-flavored tobacco ban in California found that while SB 793 was effective in reducing some types of flavored tobacco use (combustible cigarettes, cigars and smokeless tobacco), flavored e-cigarette use in adolescents was unchanged stressing the need to continue to focus public health efforts in this population group6. Other studies similarly found that SB 793 had not impacted adolescent on-line sales of e-cigarettes in California7; and the 2024 California Youth Tobacco Survey found that high school students were continuing to purchase e-cigarettes from tobacco, smoke and vape shops (12th graders) compared with 10th grade students who sourced them most often from other individuals1.
COVID-19
SB 793 was passed approximately 2 years after the COVID-19 pandemic ‘stay at home’ orders, which some studies suggested resulted in a decreased use of tobacco products early in the pandemic8, but returned to pre-pandemic levels by 2021 and 20229. Any future interventions targeting SHS, SHA and tobacco product use, may benefit from thinking about exposures in the context of being in the post-COVID-19 era.
Using two established birth cohorts of primarily low socioeconomic status, foreign-born, Spanish-speaking Latina mothers and US-born Latino middle and high school adolescents in the greater San Francisco Bay Area, we sought to evaluate attitudes and practices of ENDS product and combustible cigarette use and SHS and SHA exposures in 2023 and 2024, after the implementation of SB 793. Second, we evaluated whether COVID-19 impacted any beliefs or attitudes towards use of tobacco products and SHS and SHA exposures as described below.
METHODS
We conducted a cross-sectional survey of 115 Latina mothers, 50 high school children, and 30 middle school students on questions related to tobacco product use and SHS and SHA exposure using two previously recruited cohorts of San Francisco based-Latino mothers and children. Specifics of cohort recruitment and demographics collected have been previously described10,11. In short, pregnant Latina women were recruited at two San Francisco hospitals, University of California, San Francisco (UCSF) and Zuckerberg San Francisco General Hospital (ZSFG). We collected demographics on the participants at cohort recruitment including the following: language used at home (Spanish vs English, or English with Spanish); Special Supplemental Nutrition Program for Women, Infants and Children (WIC) participation during pregnancy (yes, no); maternal education level (high school or lower vs any college or higher), maternal age at the time of delivery (continuous and categorical with groupings as follows: 18–24, 25–30, or >30 years); residency in the US (<5, 5–15, >15 years), and child sex at birth (male, female). During the COVID-19 pandemic (2020 and 2021), families were re-contacted and questions were asked about number of individuals living in the household (continuous count and the following groupings: 1–3, 4–5 and ≥6) and maternal employment status (yes, no)12.
Participants were re-contacted by phone in 2023 and 2024, and mothers and children were invited to participate in this study which included asking questions from three validated surveys over the phone. Each interview took approximately 20 minutes and was conducted either in English or Spanish depending on the participant’s choice. The following surveys were used in the interview: 1) Adult Secondhand Exposure to Smoke (ASHES) questionnaire13, which focused on self-reported exposures to SHS and SHA (from any ENDS product) in different settings during two time periods – the last 24 hours and the last seven days – as well as an open-ended question that asked where any exposures had occurred; 2) Adolescent Smoking Consequences Questionnaire (ASCQ)14, which focused on consequences related to smoking cigarettes, with responses scaled from 1 (never) to 5 (always). All questionnaires have been previously validated with good measures of internal consistency. Additional questions were asked that assessed current tobacco use status, knowledge related to California Senate Bill 7933 and questions about any behavior changes with regard to SHS and SHA in relation to COVID-19. Child age at interview was also collected (in years) and current maternal and child tobacco product use.
To describe the sample, we calculated frequencies and percentages, and mean and standard deviation (SD) in relation to family and child demographics. Means and standard deviations were used to describe mother’s years in the US, the number of people in the home, child age, and mothers’ age at delivery.
Four groups were used as exposures for the study: high school students, middle school students, mothers of high school students, and mothers of middle school students. Several outcomes were measured, including self-reported tobacco use and attitudes to SHS and SHA, behavior changes related to changes in California legislation (SB 793), and beliefs regarding smoking, SHS and SHA, and the risk of COVID-19 and severe COVID-19. We did not analyze all portions of the ASHES or ASCQ, and as such no sub-scores or total scores were assessed. The study was approved by the Institutional Review Board (IRB) at the University of California, San Francisco (UCSF) and all mothers provided written consent for their and their children’s participation, and children gave assent to their participation.
Statistical analysis
We used chi-squared and Student’s t-test and Fisher’s exact test to compare attitudes and beliefs between mothers and children in the high school versus middle school groups. All statistical tests were two-tailed, and comparisons between mothers and children were conducted separately for high school versus middle school samples. All analyses were conducted using R Studio version 2024.9.0.375 and Stata 18.0. Statistical significance was set for all analyses at p<0.05.
RESULTS
Sample demographics
A total of 115 mother and child pairs including 30 middle school and 50 high school students, respectively, were included in this study. The majority of mothers in both the high school group and the middle school groups primarily spoke Spanish at home (90.7% and 95.0%, respectively), with a small proportion speaking English (9.3% and 5.0%, respectively) (Table 1). High school student households tended to have a greater number of individuals living in the home than middle school families with more households with ≥6 individuals versus middle school households (30.8% vs 17.9%; p<0.01) (Table 1). Mothers of high school students were also older (29.3 ± 5.7 vs 25.9 ± 5.1 years, p=0.002) than those of middle school students at the birth of their child and more likely to be employed (50.0% vs 6.7%, p<0.01) (Table 1). Most mothers in the high school sample (89.39%) and almost all mothers in the middle school group (97.50%) utilized the WIC program during pregnancy (Table 1). A small percentage of both groups of mothers reported any smoking or use of tobacco products: 5.3% of high and 5.0% of middle school mothers. Similarly, a low percentage of children reported any smoking or use of tobacco products (2% of high and 0% of middle school students). The cohort of students was 42.7% and 56.7% female for middle and high school students, respectively, with the mean age of middle school students 11.11 ± 0.37 years versus 17.06 ± 0.27 years for high school students.
Table 1
Maternal and child demographics (N =115)
| Variables | High school group (N=75) | Middle school group (N=40) | p* |
|---|---|---|---|
| n (%) | n (%) | ||
| Family household variables | |||
| Home language | |||
| English or Spanish/English | 7 (9.3) | 2 (5.0) | 0.493 |
| Spanish | 68 (90.7) | 38 (95.0) | |
| People in the home | 0.001 | ||
| Mean ± SD | 4.9 ± 1.4 | 4.4 ± 2.3 | 0.17 |
| 1–3 | 9 (13.8) | 19 (48.7) | <0.001 |
| 4–5 | 36 (55.4) | 13 (33.3) | 0.027 |
| ≥6 | 20 (30.8) | 7 (17.9) | 0.170 |
| Maternal variables | |||
| Age at delivery (enrollment) (years) | 0.008 | ||
| Mean ± SD | 25.9 ± 5.1 | 29.3 ± 5.7 | 0.002 |
| 18–24 | 37 (49.3) | 8 (20.5) | 0.049 |
| 25–30 | 22 (29.3) | 15 (38.7) | 0.069 |
| >30 | 16 (21.3) | 16 (41.0) | 0.001 |
| Current smoker | |||
| Yes | 4 (5.3) | 2 (5.0) | 1.000 |
| No | 71 (94.7) | 38 (95.0) | |
| Education level | |||
| High school or lower | 58 (78.4) | 33 (84.6) | 0.467 |
| Any college or higher (graduate school or degree) | 16 (21.6) | 6 (15.4) | |
| Employment | |||
| Yes | 5 (6.7) | 20 (50) | <0.001 |
| No | 70 (93.3) | 20 (50) | |
| WIC participation in pregnancy | |||
| Yes | 59 (89.4) | 39 (97.5) | 0.254 |
| No | 7 (10.6) | 1 (2.5) | |
| Years in the US at birth of child | |||
| <5 | 15 (20) | 6 (20) | 1.000 |
| 5–15 | 44 (58.7) | 19 (63.3) | 0.826 |
| >15 | 16 (21.3) | 5 (16.7) | 0.788 |
| Child variables | |||
| Age at interview (years), mean ± SD | 11.11 ± 0.37 | 17.06 ± 0.27 | <0.01 |
| Any self-reported tobacco use | |||
| Yes | 1 (2) | 0 (0) | 1.000 |
| No | 49 (98) | 30 (100) | |
| Sex at birth | |||
| Male | 43 (57.3) | 13 (43.3) | 0.204 |
| Female | 32 (42.7) | 17 (56.7) |
Self-reported tobacco use and attitudes to secondhand smoke and aerosol exposures
There were no statistically significant differences between high school children and parents in terms of having friends or family members who used tobacco products, while middle school students had fewer friends that were smokers compared with their mothers (0% vs 37.5% respectively) (Table 2). High school students (34%) were more likely to allow others to use tobacco products around them (including ENDS products) at school, when compared to the frequency their mothers (12%), allowed others to use tobacco products around them at work (p<0.01) (Table 2 and Figure 1).
Table 2
Maternal and child characteristics and attitudes and behavior related to smoking and secondhand smoke (SHS) and aerosol (SHA) exposures (N=115)
| Variables | High school group (N=75) | Middle school group (N=40) | ||||
|---|---|---|---|---|---|---|
| Maternal n (%) | Child n (%) | p* | Maternal n (%) | Child n (%) | p* | |
| Smoking demographics | ||||||
| Total number of smokers in social and family circles | ||||||
| Family members (at least 1) | 14 (18.7) | 11 (14.7) | 0.48 | 7 (17.5) | 3 (10) | 0.29 |
| Friends (at least 1) | 24 (32.0) | 18 (24.0) | 0.10 | 15 (37.5) | 0 (0) | <0.001 |
| Rules about tobacco use in house/apartment building | ||||||
| No use anywhere | 63 (87.5) | 45 (90) | 0.78 | 33 (82.5) | 27 (90) | 0.50 |
| Some use is allowed | 9 (12.5) | 5 (10) | 7 (17.5) | 3 (10) | ||
| SHS and SHA exposures | ||||||
| Self-reported exposures last 7 days to SHS or SHA | ||||||
| Home | 4 (5.3) | 5 (10) | 0.482 | 5 (12.5) | 2 (6.7) | 0.691 |
| Public place | 32 (42) | 26 (52) | 0.39 | 21 (52.5) | 13 (43.3) | 0.478 |
| Bus/car | 8 (10.5) | 10 (30) | 0.7 | 2 (5) | 0 (0) | |
| School | 12 (24) | 0 (0) | ||||
| Other | 18 (24) | 18 (36) | 0.509 | 16 (40) | 10 (33.3) | 0.624 |
| Self-reported exposures last 24 hours to SHS or SHA | ||||||
| Home | 3 (4) | 1 (2) | 0.649 | 4 (10) | 1 (3.3) | 0.383 |
| Bus/car/public place | 15 (197) | 5 (10) | 0.239 | 7 (23.0) | 2 (7.1) | 0.397 |
| Attitudes to SHS and SHA | ||||||
| Allow others to use tobacco products around you at home | ||||||
| Yes/sometimes | 0 (0) | 2 (4) | 0.158 | 2 (5) | 1 (3.3) | 1 |
| No/never | 75 (100) | 48 (96) | 38 (95) | 29 (96.7) | ||
| Allow others to use tobacco products around you at school/work | ||||||
| Yes/sometimes | 9 (12.0) | 17 (34.0) | <0.01 | 2 (5) | 2 (6.7) | 1 |
| No/never | 66 (88.0) | 33 (66.0) | 38 (95.0) | 28 (93.3) | ||
| Avoid smoke around you (move away) | ||||||
| Always | 65 (86.7) | 38 (76.0) | 0.153 | 37 (92.5) | 28 (93.3) | 1 |
| Sometimes/never | 10 (13.3) | 12 (24.0) | 3 (7.5) | 2 (6.7) | ||
| Avoid aerosol from ENDS around you (move away) | ||||||
| Always | 66 (88.0) | 37 (74.0) | 0.056 | 37 (92.5) | 29 (96.7) | 0.63 |
| Sometimes/never | 9 (12.0) | 13 (26.0) | 3 (7.5) | 1 (3.3) | ||
| Move away from smoke/aerosol around you | ||||||
| Always | 66 (88.0) | 35 (70.0) | 0.02 | 37 (92.5) | 28 (93.3) | 1 |
| Sometimes/never | 9 (12.0) | 15 (30.0) | 3 (7.5) | 2 (6.7) | ||
| Move away from smoke in the park | ||||||
| Always | 69 (93.2) | 45 (90.0) | 0.754 | 37 (92.5) | 28 (93.3) | 1 |
| Sometimes/never | 6 (8.1) | 5 (10.0) | 3 (7.5) | 2 (6.7) | ||
| Move away from aerosol in the park | ||||||
| Always | 68 (90.7) | 43 (86.0) | 0.564 | 37 (92.5) | 28 (93.3) | 1 |
| Sometimes/never | 7 (9.3) | 7 (14.0) | 3 (7.5) | 2 (6.7) | ||
| COVID and attitudes to smoking and vaping | ||||||
| Believes smoking is more dangerous now because of COVID | ||||||
| Always | 49 (68.1) | 24 (48) | 0.038 | 28 (70.0) | 22 (73.3) | 0.796 |
| Sometimes/never | 23 (31.9) | 26 (52) | 12 (30.0) | 8 (26.7) | ||
| Believes smoking + ENDS increases risk of severe COVID | ||||||
| Always | 41 (57.8) | 17 (34) | 0.016 | 23 (60.5) | 19 (63.3) | 0.244 |
| Sometimes/never | 30 (42.3) | 33 (66) | 15 (39.5) | 11 (36.7) | ||
| Believes SHS can make it easier to get COVID | ||||||
| Always | 28 (37.3) | 12 (24) | 0.170 | 16 (40) | 11 (36.7) | 0.809 |
| Sometimes/never | 47 (62.7) | 38 (76) | 24 (60) | 19 (63.3) | ||
| Believes exposure to SHA can make it easier to get COVID | ||||||
| Always | 27 (36) | 12 (24) | 0.173 | 14 (35) | 12 (40) | 0.8033 |
| Sometimes/never | 48 (64) | 38 (76) | 26 (65) | 18 (60) | ||
| Attitudes towards SB 793 | ||||||
| Agrees with law prohibiting flavored tobacco sales | ||||||
| Always | 63 (84) | 40 (81.6) | 0.808 | 32 (80) | 26 (86.7) | 0.536 |
| Sometimes/never | 12 (16) | 9 (18.4) | 8 (20) | 4 (13.3) | ||
| Believes it is still possible to purchase flavored tobacco products even with SB 793 | ||||||
| Always | 36 (50) | 26 (53.1) | 0.853 | 20 (54.1) | 6 (20) | 0.005 |
| Sometimes/never | 36 (50) | 23 (46.9) | 17 (45.9) | 24 (80) | ||
| Uses flavored tobacco products less with change in law in California | ||||||
| Always | 35 (74.5) | 20 (48.8) | 0.016 | 29 (90.6) | 20 (76.9) | 0.274 |
| Sometimes/never | 12 (25.5) | 21 (51.2) | 3 (9.4) | 6 (23.1) | ||
| Friends use flavored tobacco products less with change in law in California | ||||||
| Always | 31 (59.6) | 17 (34.7) | 0.017 | 29 (80.5) | 21 (77.8) | 1 |
| Sometimes/never | 21 (39.6) | 32 (65.3) | 7 (19.4) | 6 (22.2) | ||
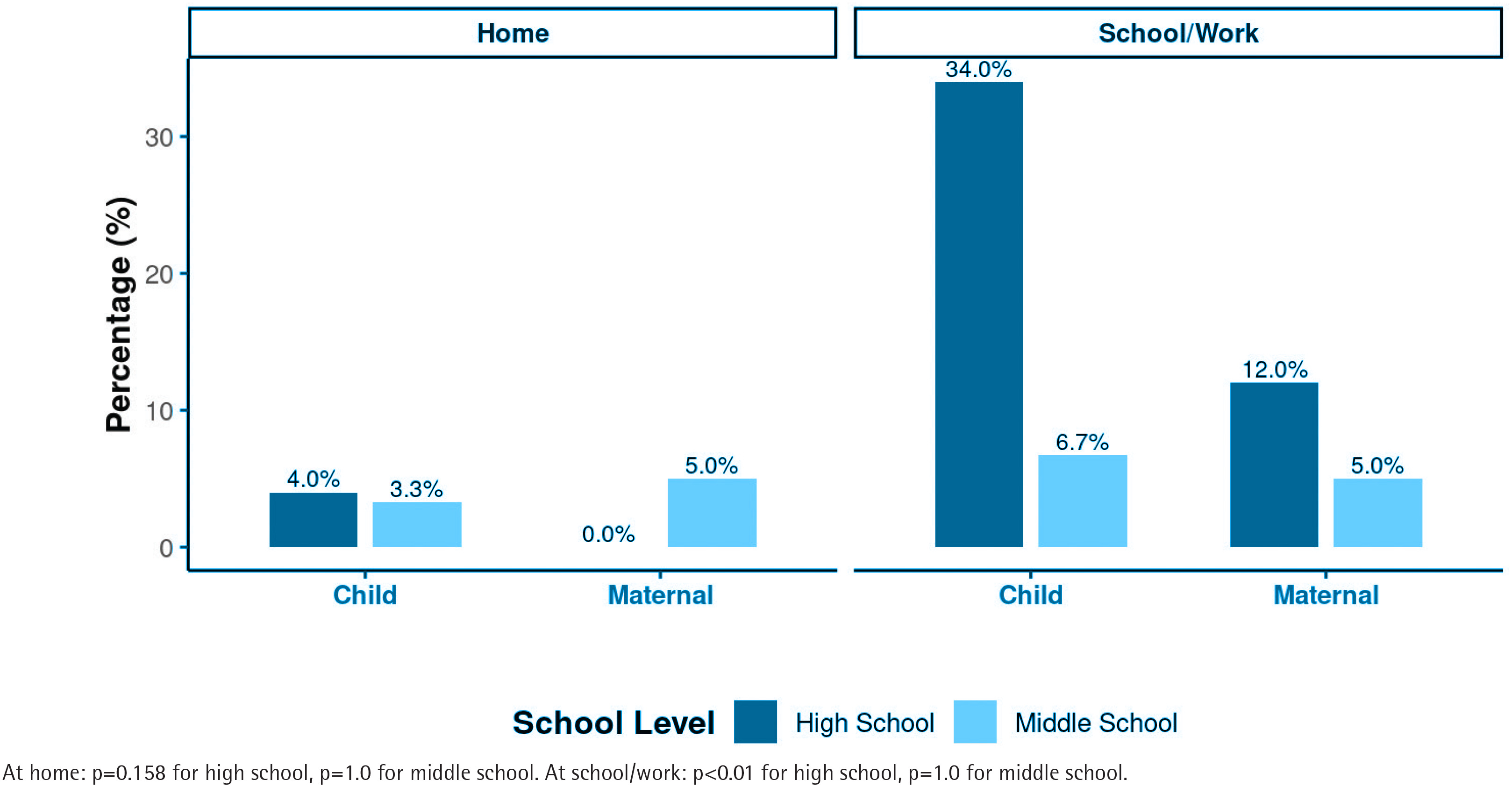
Middle school students were similar to their mothers in terms of not allowing anyone to use tobacco products around them (95.0% vs 93.3%, p=1.0). Although we did not find any statistically significant differences between 7-day exposure to SHS and SHA between mothers and children for either high or middle school students, a high percentage of high school students (67%) who cited other exposures indicated that all these exposures happened at school (in the bathrooms or walkways). Conversely, mothers and middle school students indicated that their other exposures to SHS and SHA happened in the street or other outdoor venues, and none indicated that it was at school or work.
High school students were less likely to always avoid aerosol exposure compared to their mothers (74.0% vs 88.0%, p=0.056) (Table 2) although the results did not meet statistical significance. However, mothers of high school students were more likely to move away from SHS and/or SHA than their children (88.0% vs 70.0%, p=0.02) (Table 2). There were no statistically significant differences between middle school students and mothers in regard to SHS or SHA avoidance. Both reported a high rate of avoidance (92.5% and 96.7%, respectively, for SHA, and 92.5% and 93.3%, respectively, for avoidance of SHS and/or SHA (Table 2).
Beliefs regarding use of tobacco products and risk of COVID-19
Mothers of high school students were more likely than high school students to believe that use of tobacco products is more dangerous in the context of COVID-19 (68.1% of mothers versus 48.0% of students, p=0.038). Similarly, mothers of high school students were also more likely to believe that smoking and using of ENDS product increase the risk of developing severe COVID-19 (57.8% of mothers, versus 34% of students, p=0.016). There was no difference between mothers of middle school students and middle school students on beliefs about the impact of tobacco product use on risk of COVID-19 and severe COVID-19. (Table 2)
Legislation in California (SB 793) and behavior changes related to legislation
A high percentage of high and middle school students and their mothers agreed with SB 793, banning the sale of flavored tobacco products (84.0% of mothers of high school and 80.0% of mothers of middle school students; 81.6% of high school and 86.7% of middle school students) (Table 2). However, high school students did not think that SB 793 would change use patterns of flavored tobacco products for themselves or any friends compared with their mothers (51.2% of students believed the law would not be impactful, and 65.3% believed it would not be impactful for friends), compared with 25.5% of mothers who thought the impact would be minimal impactful for themselves or 39.6% for friends (p=0.016 and p=0.017, respectively) (Table 2).
DISCUSSION
In this study of SHS and SHA exposures, we found approximately half of high school students and slightly less than half of middle school students had weekly exposures comparable with national level data from the 2015–2017 National Youth Tobacco Survey5. The on-going high level of exposure for students indicates an urgent need to focus on smoke and aerosol-free environments particularly in outdoor settings for Californians. Additionally, a high percentage of high school students reported SHS and/or SHA exposures compared with middle school students, particularly within school settings such as bathrooms, hallways, and outdoors areas. Similarly, a higher percentage of high school students indicated that they allowed others to use tobacco products around them at school than did middle school students or their parents. The high school students in our study were significantly older (17 years) versus the middle school students (11 years) and other studies have found a much higher percentage of tobacco product use among high versus middle school students15, as well as an accelerated increase of e-cigarette initiation from 11 to 17 years of age16.
SB 793
Although SB 793 now prohibits the sale of flavored tobacco products in California, high school students surveyed often stated that the bill would make no difference for themselves or their peers in terms of having access to flavored tobacco products. High school students noted that they were able to obtain flavored vapes from other places, including from friends, online and smoke shops that continue to sell flavored tobacco products despite the new law. By contrast middle school students believed in the efficacy of the law to prevent flavored tobacco sales.
The ability for Bay Area high schoolers to easily access flavored tobacco products has been confirmed in studies from other parts of California. In a recent study more than half of flavored tobacco online transactions in San Diego were still delivered in spite of SB 793 and citywide ordinances preventing online sales of flavored tobacco17. San Francisco similarly has had an ordinance that bans online and mail order of flavored tobacco products since 2017, and recently sued Rogue Holdings, Swisher International and Northern Scandinavia for violating the ban and selling flavored Zyns (tobacco pouches) online18. California passed AB 3218 and SB 1230 in 2024 explicitly forbidding flavored tobacco online sales to ensure a further reduction in flavored tobacco use as online sales were not specifically mentioned in SB 79319. Meanwhile, we found two online sites that were advertising the sale of flavored tobacco products in SF20,21.
COVID-19
High school students were less concerned about any interactions between SHS and SHA exposures and COVID-19 risk and severity of disease, compared with mothers and middle school students. Previous studies have found that SHS and SHA exposure is associated with more severe COVID-19 infection22, and it may be helpful in future educational campaigns to stress the risk associated with subsequent health issues including COVID-19 before students enter high school, prior to any initiation of tobacco use products23.
Limitations
Limitations of this study include a small sample size and the inability to conduct any adjusted analyses. However, our population was relatively homogenous in terms of country of origin, participation in WIC and overall socioeconomic status10,11. Additionally, the focus of the study was on Spanish-speaking mothers and their US-born children in the San Francisco Bay Area, which may limit the generalizability of our findings to other populations including other Latino populations in the state of California. Lastly, as the study was cross-sectional, we were unable to determine causality between exposures, and self-reported data may have resulted in misclassification bias although the direction of the bias would have been non-differential.
CONCLUSIONS
Additional studies are needed to assess SHA and SHS exposures in multi-racial and ethnic cohorts, as we assessed only Latino, US-born students and their predominantly foreign-born mothers. Future interventions should also focus on the early years of high school to prevent initiation, and work with school districts to prevent bathroom, hallway and other exposure areas during the school day. Other studies and interventions also need to ensure that online, and brick and mortar retailers comply with statewide and municipal legislation, and continue to monitor how and where students are accessing tobacco products.