
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a type of heterogeneous lung disease characterized by chronic respiratory symptoms (such as dyspnea, cough, and sputum production or exacerbation) that are caused by abnormalities in the airways and/or alveoli, leading to persistent airflow limitation1. The social burden of COPD is generally measured by incidence, mortality, and disability-adjusted life years (DALYs). The global prevalence of COPD in people aged > 40 years is over 9–10%, and these data are usually derived from statistics of various medical data, including doctor visits, emergency visits, and hospitalization records2-4. In 2019, a global report documented 212.3 million cases of COPD, with 3.3 million deaths, and a global ASMR of 42.5 (95% UI: 37.6–46.3)5, making COPD the third leading cause of death worldwide6. DALYs refer to the entire number of healthy life years lost due to the disease from the onset of the disease to the end of death (or survival at the time of evaluation) due to the disease7. From 1990 to 2019, COPD was a major contributor to the increase in global DALYs, with COPD-related DALYs increasing by 25.7%. In 2019, the global ASDR for COPD was 926.1 (95% UI: 848.8–997.7). The DALY rate and mortality rate of COPD patients vary by region, with Oceania having the highest ASMR (112.1) and ASDR (2309.9) from COPD5. From 1990 to 2019, Southeast Asia, India, Sub-Saharan Africa, and the Americas saw the largest increases in ASDR5,8,9. The high incidence, high mortality, and high DALY rates of COPD have resulted in a significant economic burden. Research on major world economies has revealed that COPD costs account for approximately 56% (386 billion euros) of respiratory disease costs in the European Union1. COPD costs in the United States are expected to continue to rise over the next 20 years, with estimated total costs of around $800.9 billion1. The median direct medical cost for Chinese COPD patients is $150 to $2014 per person per year10. Improving the prevention and treatment levels of COPD patients is an essential aspect of reducing the global disease burden. Shifting the diagnostic gateway of COPD is a key measure to improve the prevention and treatment level of COPD, which is of great significance in delaying the progression, improving prognosis, and reducing the disease burden of COPD11,12. Moreover, regularly assessing the global disease burden of COPD patients, timely understanding the dynamic changes of the global disease burden of COPD, and adjusting and improving existing prevention and treatment strategies promptly are also crucial for reducing the disease burden of COPD.
At the end of 2019, the outbreak of COVID-19 changed the medical practice of the entire world13. For COPD patients, the COVID-19 pandemic had greatly affected routine management, diagnosis, and treatment activities of COPD. Epidemiological surveys have revealed that COPD patients were a major risk group for infection with the SARS-CoV-2. Compared to non-COPD patients, COPD patients have a significantly increased risk of ICU admission and a roughly 2.5 times higher risk of death14. Although the COVID-19 epidemic has been effectively controlled, some countries and regions continue to report new cases and deaths of COVID-1915. This indicates that COPD patients may be affected by SARS-CoV-2 for a long time, so the analysis of the burden of COPD disease during the COVID-19 period is extremely valuable. Based on data from the GBD 2021 study, we comprehensively analyzed variations in the incidence, prevalence, deaths, and DALYs associated with COPD during the initial two years after the pandemic emerged.
Notably, among the various risk factors for COPD, tobacco exposure is closely associated with the onset, progression, and mortality risk of the disease and represents one of the most important and modifiable risk factors. In addition to active smoking, secondhand smoke exposure has also been linked to chronic respiratory inflammation, declines in lung function, and an increased risk of adverse COPD-related outcomes16.
Previous studies have shown that smoking increases the risk of developing COPD among middle-aged adults within five years, and that these individuals also face a higher risk of severe exacerbations and premature mortality over a 40-year period17. Moreover, evidence suggests that cigarette smoke may attenuate the anti-inflammatory effects of inhaled corticosteroids, thereby reducing treatment responsiveness in patients with COPD and leading to unfavorable outcomes18. On the other hand, a study by Osman et al.19 reported a significant association between secondhand smoke exposure and worsening health status in patients with COPD19, further highlighting the detrimental impact of cigarette smoke on COPD. Therefore, while assessing the overall burden of COPD, it is essential to further quantify the contributions of active and passive smoking to COPD-related mortality and DALYs, which is critical for interpreting changes in disease burden and for informing more targeted prevention and control strategies.
METHODS
Overview and data collection
This secondary dataset analysis was approved by the Ethics Committee of the First Hospital of Jiaxing (Ethics Number: 2024-KY-589; Date: 12 July 2024). The Ethics Committee of the First Hospital of Jiaxing agreed to waive informed consent as the study only involved data analysis without identifiable personal information.
Existing data on COPD, standardized disease definitions, and prevalence information were collected using the Global Burden of Disease Collaborator’s Global Health Data Exchange query tool. The most recent update of the GBD database was on 16 May 2024. The latest version of the GBD database assessed the morbidity, mortality, and DALYs of 371 diseases and injuries in 204 countries and territories from 1990 to 2021, providing corresponding estimates and uncertainty intervals2,20. In this study, we examined the latest updated data and collected data on COPD incidence, prevalence, and deaths and DALYs from COPD, and their respective age-standardized rate (ASR) globally, regionally, and nationally. We also collected data on global risk factors contributing to COPD-related mortality rates. This work followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines21 (Supplementary file).
Sociodemographic index
The SDI is a composite index mainly composed of three key elements: income level, education level, and fertility rate, aiming to provide a standardized way to compare the differences in social and demographic characteristics among different countries and regions and to measure the social and demographic development status of a country or region22. The range of SDI values is from 0 to 1, where 0 represents the lowest level of sociodemographic development and 1 represents the highest level of development2.
Statistical analysis
The number of incident cases, deaths, DALYs, and their corresponding rates are the main indicators describing the burden of COPD. According to the GBD algorithm, each rate is reported per 100000 people, along with a 95% UI. In the GBD framework, uncertainty intervals (UIs) are reported to capture both sampling error and model-based uncertainty. For each quantity estimated, the GBD modeling process generates 1000 posterior draws. The 2.5th and 97.5th percentiles of the ordered draws are then taken as the lower and upper limits of the 95% UI23. Thus, all point estimates in our study, including incidence, prevalence, mortality and DALYs, are accompanied by their 95% UIs to ensure transparent presentation of uncertainty associated with data sparsity and modeling. The dynamics of COPD are analyzed by calculating estimated annual percentage changes (EAPCs) to determine the time trends of disease burden. The linear modeling is applied to determine the 95% confidence interval (95% CI) of EAPCs24. When both the EAPCs and their 95% CI upper limits are negative, the corresponding rates show a decreasing trend. Conversely, if both the EAPC and their 95% CI lower limits are positive, the corresponding rates show an increasing trend. In addition, if the 95% CI of the EAPC includes 0, it indicates that the change is not statistically significant22. We used Spearman rank correlation and linear regression analysis to explore the relationship of SDI with ASMR and ASDR in COPD patients25. In this study, the R software package (version4.2.3) and JD_GBDR (V2.22, Jingding Medical Technology Co., Ltd.) were used for the drawing of the figures.
RESULTS
Global trends
In 2021, the global number of COPD cases was 16.9 million (95% UI: 15.5–18.3 million), with the ASIR of 197.37 (95% UI: 181.65–213.42). Compared to 2019, there was no significant change in the global ASIR of COPD in 2021 [2019: 197.30 (95% UI: 181.85–213.09); EAPCs: 0.02 (95% CI: -1.08–1.14)] (Supplementary file Table S1). In 2021, the number of COPD cases reached 213 million (95% UI: 195–234 million), with an ASPR of 2512.86 (95% UI: 2293.93–2748.52). The ASPR slightly decreased compared to 2019 [2019: 2520.67 (95% UI: 2306.51–2756.83); EAPCs: -0.15 (95% CI: -1.54–1.25)] (Supplementary file Table S2).
In 2021, COPD resulted in 3.72 million deaths (95% UI: 3.35–4.08 million), with the corresponding ASMR decreasing from 46.09 in 2019 (95% UI: 41.81–49.66) to 45.22 in 2021 (95% UI: 40.61–49.70), with EAPCs of -0.95 (95% CI: -2.70–0.83) (Table 1).
Table 1
The deaths and ASMR from COPD in 2019 and 2021, at global and regional levels
In 2021, the estimated number of DALYs due to COPD was 79.78 million (95% UI: 74.03–86.01), with an ASDR of 940.66 (95% UI: 871.48–1014.59), a decrease compared to 2019 [2019: 958.62 (95% UI: 889.80–1023.31); EAPCs: -0.94 (95% CI: -2.99–1.15)] (Supplementary file Table S3).
SDI trends
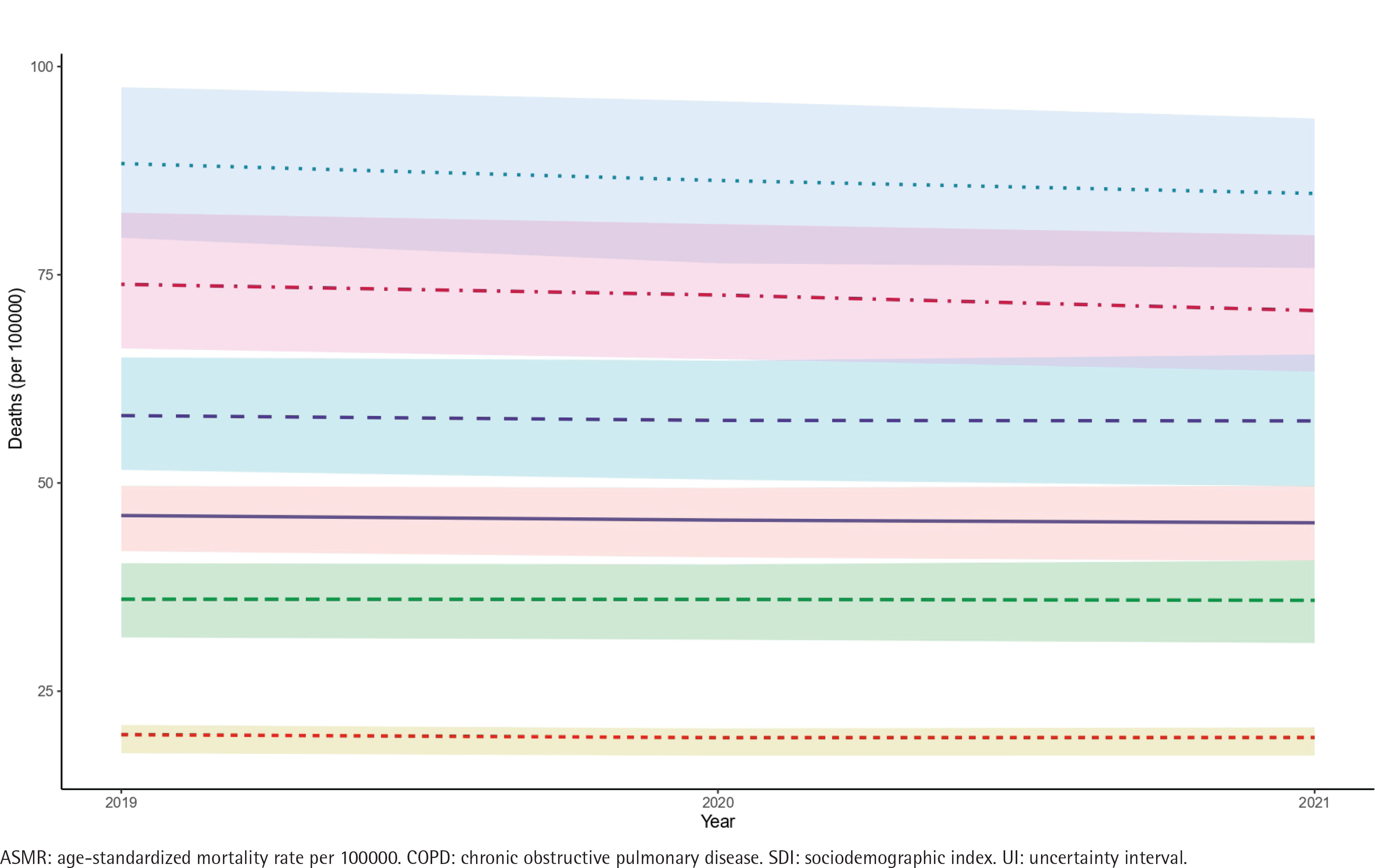
In 2021, the COPD disease burden exhibited significant regional differences. Among the five SDI regions, the low-middle SDI region had the highest ASIR, ASPR, ASMR, and ASDR, with rates of 227.24 (95% UI: 212.55–242.96), 2726.76 (95% UI: 2478.22–2,979.00), 84.76 (95% UI: 75.80–93.78), and 1707.90 (95% UI: 1558.88–1865.11), respectively. The highest number of COPD cases, deaths, and DALYs were observed in the middle SDI region, with 5.33 million cases (95% UI: 4.82–5.86 million), 63.93 million cases (95% UI: 57.32–71.32 million), 1.29 million deaths (95% UI: 1.12–1.48 million), and 26.68 million DALYs (95% UI, 23.96–29.74 million). The high-middle SDI region had the lowest ASIR, the low SDI region had the lowest ASPR, while the high SDI region had the lowest ASMR and ASDR. From 2019 to 2021, the ASMR and ASDR showed a slight downward trend across all five SDI regions, with EAPCs all being less than 0 (Table 1, Figure 1; and Supplementary file Figures S1–S3).
Geographical regional trends
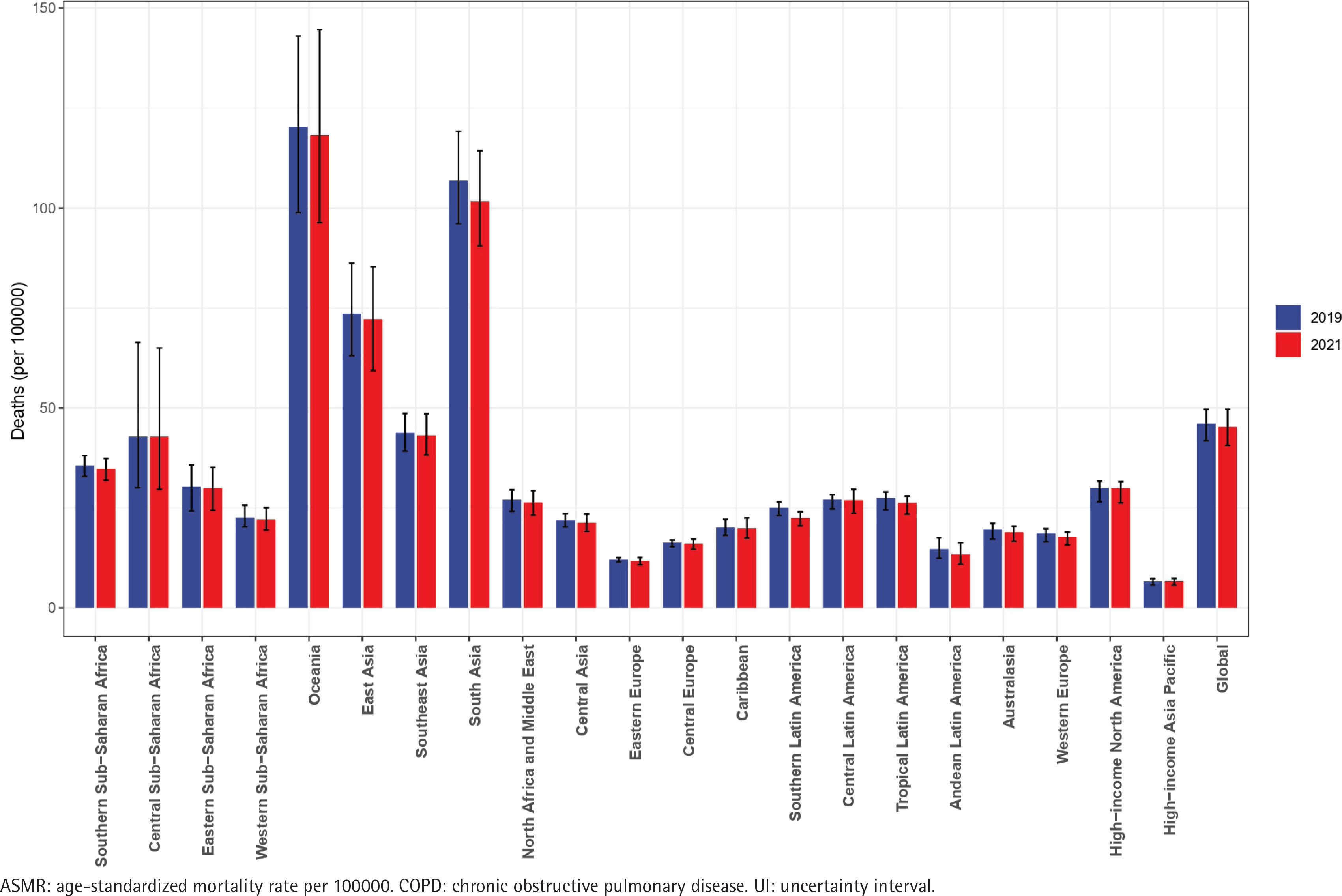
Among the 21 geographical regions, East Asia had the highest number of COPD cases, prevalence, and deaths, with 4.57 million cases (95% UI: 4.13–5.00 million), 52.09 million cases (95% UI: 46.32–58.80 million), and 1.32 million deaths (95% UI: 1.08–1.57 million), respectively. South Asia had the highest number of DALYs, with 28.01 million (95% UI: 25.40–30.94 million). In addition, South Asia also had the highest ASIR at 258.26 (95% UI: 242.49–273.76), and High-income North America had the highest ASPR, at 3298.88 (95% UI: 3132.14–3451.88). The three regions with the highest ASMR were Oceania [118.21 (95% UI: 96.32–144.59)], South Asia [101.63 (95% UI: 90.55–114.34)], and East Asia [72.20 (95% UI: 59.32–85.26)]. The regions with the highest ASDR were also the same three: [Oceania: 2351.49 (95% UI: 1931.26–2854.06), South Asia: 2049.22 (95% UI: 1862.71–2268.73), and East Asia: 1217.69 (95% UI: 1043.87–1422.79)].
From 2019 to 2021, the ASMR in all 21 geographical regions decreased compared to 2019, and the ASDR decreased in all regions except Central Latin America and Central Sub-Saharan Africa. In 2021, the ASIR and ASPR increased in Eastern Europe, Western SubSaharan Africa, Eastern Sub-Saharan Africa, Central Sub-Saharan Africa, North Africa and the Middle East, Tropical Latin America, Southeast Asia, Southern Sub-Saharan Africa, and Oceania compared to 2019 (Figure 2; and Supplementary file Figures S4–S6).
National trends
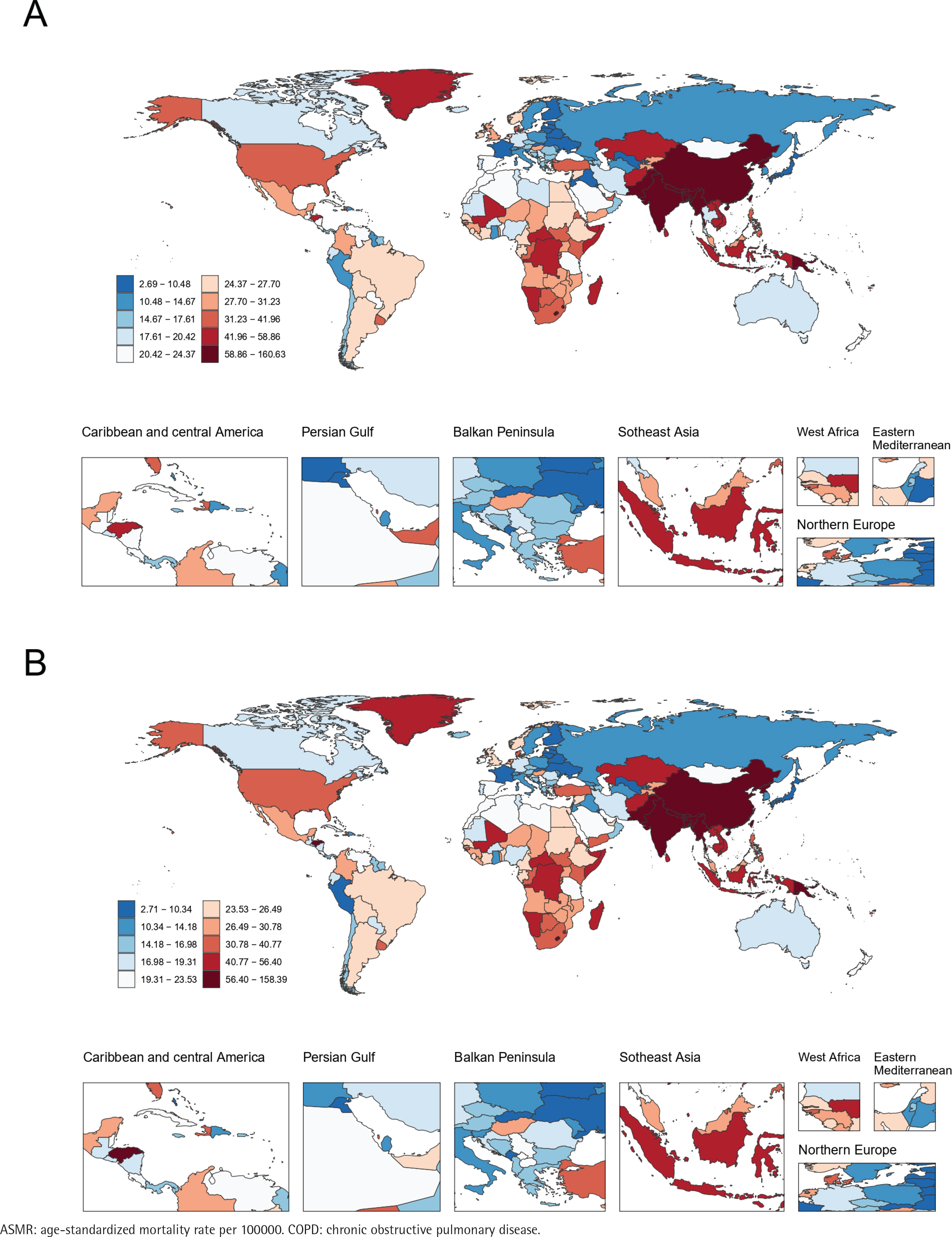
In 2021, among 204 countries and regions, China, India, and the United States had the highest numbers of cases, prevalence, deaths, and DALYs. The ASIR across countries ranged from 66.76 to 310.58. Nepal [310.58 (95% UI: 300.58–319.7)], Papua New Guinea [279.71 (95% UI: 263.93–294.94)], and India [262.45 (95% UI: 246.14–277.48)] had the highest ASIRs. The ASPR ranged from 922.56 to 3445.29, with the highest ASPRs in the United States [3445.29 (95% UI: 3263.49–3602.42)], the United Kingdom [3270.26 (95% UI: 2957.04–3570.38)], and Turkey [3146.68 (95% UI: 2861.31–3477.82)]. Papua New Guinea [ASMR: 156.82 (95% UI: 123.55–197.43), ASDR: 3004.36 (95% UI: 2404.29–3732.82)], Nepal [ASMR: 146.13 (95% UI: 116.66–182.46), ASDR: 2836.01 (95% UI: 2275.31–3485.04)], and India [ASMR: 108.39 (95% UI: 94.73–122.39), ASDR: 2171.16 (95% UI: 1953.69–2422.39)] had the highest ASMR and ASDR. The lowest ASMRs were in Kuwait [2.74 (95% UI: 2.24–3.28)], Japan [5.84 (95% UI: 4.93–6.33)], and Montenegro [5.87 (95% UI: 4.63–7.15)], while the lowest ASDRs were in Kuwait [160.46 (95% UI: 138.49–185.65)], Japan [155.76 (95% UI: 137.62–174.26)], and Singapore [146.48 (95% UI: 131.42–161.67)] (Tables 2 and 3, and Figure 3; and Supplementary file Tables S4–S7 and Figures S7–S9).
Table 2
The deaths and ASMR from COPD in the top five countries, in 2019 and 2021
Table 3
The number of DALYs and ASDR from COPD in the top five countries, in 2019 and 2021
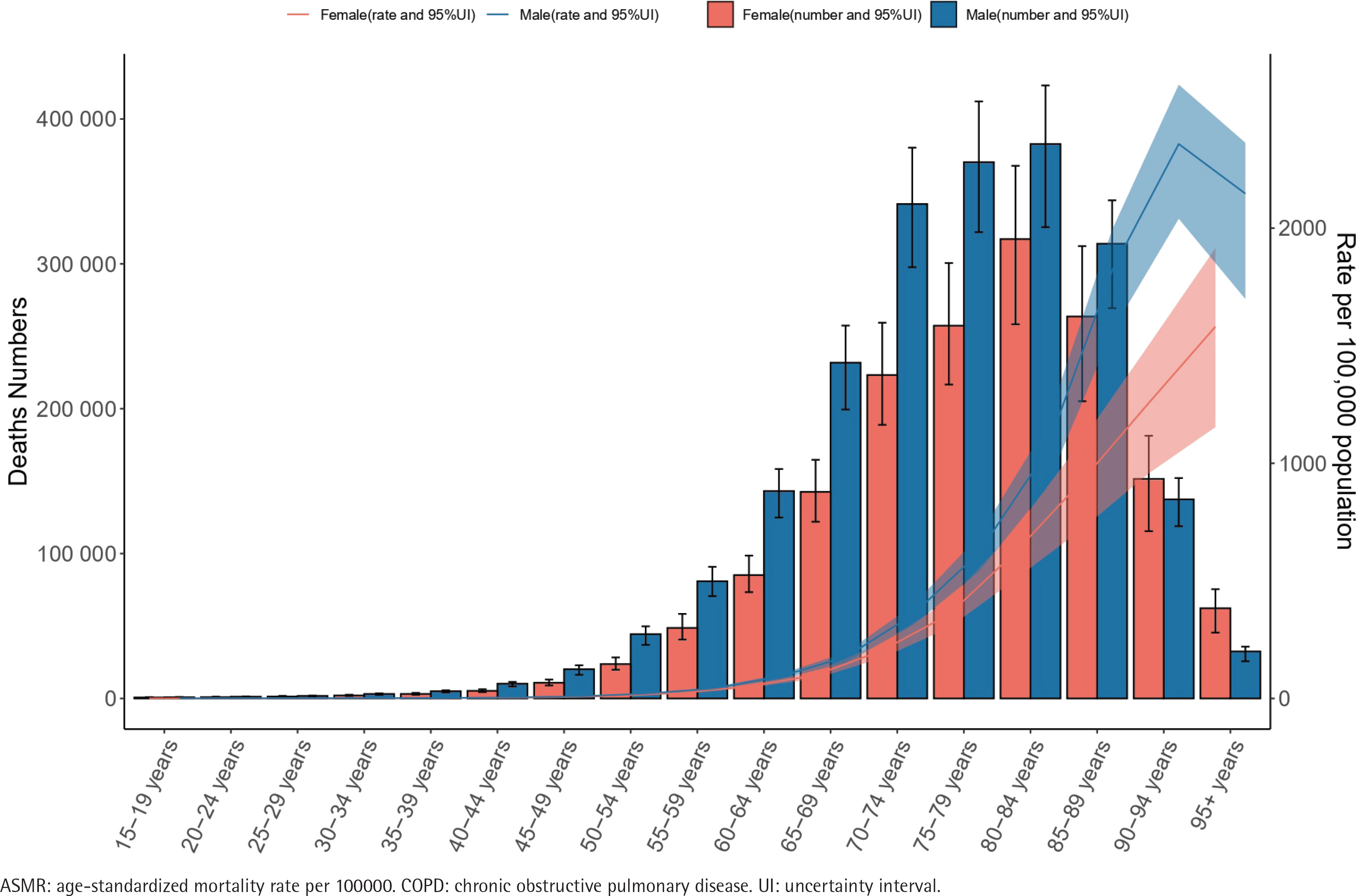
Age and sex pattern
In 2021, the ASIR, ASPR, female ASMR, and female ASDR of COPD patients increased with age, reaching their highest levels in the age group >95 years. Specifically, the ASIR was 2078.94 (95% UI: 1345.73–2835.23), ASPR was 42366.01 (95% UI: 36676.77–49170.72), female ASMR was 1581.27 (95% UI: 1153.76–1914.99), and female ASDR was 14939.34 (95% UI: 11538.17–17794.61). In contrast, male ASMR [2357.79 (95% UI: 2039.83–2610.24)] and male ASDR [22345.83 (95% UI: 19515.18–24654.34)] peaked in the 90–94 years age group (Figure 4; and Supplementary file Figures S10–S12).
Association with SDI
We found that in 2021, there was an inverted U-shaped association of SDI with ASMR and ASDR in COPD patients. As the SDI increased, the ASMR showed a trend of first increasing and then decreasing, reaching its peak at SDI of 0.45 (Supplementary file Figures S13 and S14).
Risk factors for COPD patients
In 2021, the primary risk factors for COPD-related deaths globally were ambient ozone pollution (13.06%), high temperature (0.99%), low temperature (8.16%), occupational exposure to particulate matter, gases, and fumes (15.56%), particulate matter pollution (40.95%), secondhand smoke (7.16%), and smoking (35.65%). Among these, particulate matter pollution contributed to an ASMR of 18.51 (95% UI: 14.64–23.13). Additionally, we found that the attribution risk factors varied by region. In Oceania, Western Sub-Saharan Africa, Eastern Sub-Saharan Africa, and Central Sub-Saharan Africa, the main attribution risk factors for COPD-related deaths were occupational exposure to particulate matter, gases, and fumes, and particulate matter pollution, while in Central Europe and Eastern Europe, smoking was the primary risk factor (Supplementary file Figure S15).
In further analyses of tobacco, smoking, and secondhand smoke, we found that in 2021, tobacco exposure was responsible for 1510388.83 deaths (95% UI: 1139036.41–1872108.29) and 31613440.38 DALYs (95% UI: 23984861.88–38521071.25). The corresponding ASMR and ASDR were 18.26 (95% UI: 13.77–22.67) and 370.64 (95% UI: 280.85–452.10), respectively. Smoking accounted for 1334961.49 deaths (95% UI: 1053265.31–1596644.97) and 27794778.42 DALYs (95% UI: 22233658.14–32884383.79), with an ASMR of 16.12 (95% UI: 12.68–19.29) and an ASDR of 325.52 (95% UI: 260.32–385.52). In addition, secondhand smoke exposure resulted in 266124.70 deaths (95% UI: 106054.27–434215.02), corresponding to an ASMR of 3.24 (95% UI: 1.29–5.29), and 5662904.86 DALYs (95% UI: 2246472.20–9077004.16), with an ASDR of 66.78 (95% UI: 26.50–106.98). From 2019 to 2021, the absolute numbers of deaths and DALYs attributable to tobacco increased, whereas the corresponding ASR declined over the same period. Further stratified analyses by sex showed that in 2021, the mortality attributable to tobacco was 1161715.93 (95% UI: 904881.73–1406961.20) among males and 348672.90 (95% UI: 210507.13–496540.99) among females. The mortality attributable to smoking were 1102915.41 (95% UI: 871018.69–1325061.31) for males and 232046.09 (95% UI: 163632.30–316139.31) for females, while those attributable to secondhand smoke were 131347.84 (95% UI: 51635.78–217953.09) and 134776.87 (95% UI: 51788.39–221145.99), respectively. Notably, the sex difference in mortality attributable to secondhand smoke was substantially smaller than that observed for tobacco and smoking. The DALYs attributable to tobacco, smoking, and secondhand smoke among males were 24103410.31 (95% UI: 18915059.71–28682355.15), 22843000.96 (95% UI: 18383346.15–26947224.92), and 2724515.49 (95% UI: 1095246.44–4376779.77), respectively, whereas the corresponding DALYs among females were 7510030.07 (95% UI: 4643774.76–10407607.70), 4951777.44 (95% UI: 3630190.76–6490676.81), and 2938389.37 (95% UI: 1132101.32–4747521.66) (Tables 4 and 5; and Supplementary file Figures S16 and S17).
Table 4
The deaths and ASMR from COPD attributable to tobacco and smoking, in 2019 and 2021
Table 5
The number of DALYs and ASDR from COPD attributable to tobacco and smoking, in 2019 and 2021
DISCUSSION
COPD is a major global public health problem, and the global investment in COPD prevention and treatment is increasing every year, resulting in a lot of economic and social burden to all countries26. The sudden outbreak and epidemic of COVID-19 at the end of 2019 has brought great challenges to the global management of chronic diseases, which is another global public health problem worthy of attention13. In this context, we aimed to ascertain whether the burden of COPD disease showed new trends. We analyzed the ASIR, ASPR, ASMR, ASDR, and mortality-related attribution risk factors for COPD across all GBD regions and countries during the period of COVID-19 emergence (2019–2021). However, the results were contrary to our expectations. Globally, there was no significant trend in the ASIR and ASDR of COPD from 2019 to 2021, and the ASMR and ASDR slightly decreased compared to 2019.
Previous studies have shown that COPD patients may face a higher risk of death after contracting COVID-19 due to disruptions in healthcare services and reduced routine management27. A meta-analysis by Reyes et al.28 found a significantly increased mortality rate in COPD patients infected with COVID-19, and a similar conclusion was reached by Ahn et al.29. However, our study found that the COPD disease burden did not show an upward trend from 2019 to 2021. We speculate that this may be related to several factors.
During the COVID-19 pandemic, widespread public health measures such as wearing masks, maintaining social distancing, frequent handwashing, and limiting large gatherings were implemented globally. These measures reduced the circulation of common respiratory viruses, which are important triggers for acute exacerbations of COPD30. The reduction in viral infections directly lowered the risk of exacerbations in COPD patients30-32. Secondly, statistical and reporting biases may have affected the accurate assessment of the disease burden. In the early stages of the pandemic, some COPD-related deaths were misclassified as COVID-19-related deaths33. Additionally, due to the reallocation of medical resources or the impact of public health measures, many COPD patients with mild symptoms did not seek timely medical attention, and some cases were not included in the COPD statistics, which may have led to an underestimation of the disease burden34 . On the other hand, although medical resources in some regions were redirected towards COVID-19 patients during the pandemic, the promotion of telemedicine and online consultation services provided new avenues for disease management for COPD patients, helping them continue to receive necessary medical support during the pandemic35. Additionally, factors such as the reduction in air pollution and the decline in smoking rates over the past two years may have contributed to a certain extent in reducing the COPD disease burden36.
This study further quantified the attributable burden of COPD from the perspective of tobacco-related exposures. Our findings indicate that tobacco exposure remains a major contributor to the global burden of COPD, with active smoking accounting for the dominant share; however, secondhand smoke also imposes a non-negligible burden, underscoring that protecting non-smokers and creating smoke-free environments have independent and essential roles in reducing the overall disease burden37. In terms of temporal trends, although the absolute numbers of deaths and DALYs attributable to tobacco increased between 2019 and 2021, the corresponding age-standardized rates declined. The increase in absolute burden may be attributable to global population growth and population ageing, whereas the decline in ASR likely reflects the impact of increasingly stringent tobacco control policies implemented in many countries and regions, which may have partially mitigated the COPD burden attributable to smoking38. Consistent with this interpretation, Tashkin et al.39 reported that smoking cessation can slow the decline in lung function and delay disease progression among patients with COPD39. Sex-stratified analyses further revealed that the burden attributable to active smoking was substantially higher among males, suggesting that smoking cessation interventions targeting high-risk male populations may yield greater marginal benefits. In contrast, the sex differences in ASMR and DALYs attributable to secondhand smoke were markedly smaller than those observed for tobacco and smoking, emphasizing that reducing secondhand smoke exposure relies primarily on institutional and environmental smoke-free policies rather than on individual smoking cessation alone. Moreover, previous studies have suggested that, compared with males, females may be more susceptible to the adverse effects of smoking on the development and prognosis of COPD16. Therefore, smoking and secondhand smoke exposure among women should also receive greater attention.
Limitations
This study has several limitations. First, we analyzed COPD burden based on the GBD 2021 dataset for the first two years after the COVID-19 outbreak, which may not capture the latest trends or long-term consequences, potentially underestimating the pandemic’s impact. Second, the data in the GBD database come from various sources, including national and regional reports, hospital data, and mortality statistics. The quality and coverage of these data may vary across different regions due to differences in healthcare infrastructure, diagnostic standards, reporting systems, and other factors, despite quality control, sparse or poor reporting may affect accuracy and comparability. Third, the EAPC estimates assume linear trends, which may not fully reflect nonlinear changes. Fourth, misclassification between COPD and COVID-19 deaths during 2020–2021 may have biased mortality estimates. Fifth, as an ecological study, our findings cannot be extrapolated to individuals, and the lack of stratification by COPD severity limits the assessment of disease heterogeneity. These shortcomings may affect the comprehensiveness and accuracy of the study results.
CONCLUSIONS
Our study found that the outbreak of COVID-19 does not appear to have altered the trend of COPD disease burden changes, to more accurately assess the specific effects of the pandemic on the COPD disease burden, more research should be conducted in the future. These studies should not only focus on the changes in the disease burden of COPD patients during the pandemic but also explore the long-term impact of COVID-19 on the disease burden in COPD patients. Only then can we truly understand the far-reaching effects of COVID-19 on the COPD disease burden and provide scientific evidence for the optimization of relevant prevention and control strategies. Meanwhile, in the context of the COVID-19 pandemic, smoking and tobacco exposure remain important risk factors contributing to the burden of COPD, underscoring the urgent need for heightened attention from the public and relevant authorities.