

INTRODUCTION
Smoking is the second largest risk factor for early death and associated morbidity1,2. Some populations are more sensitive to its harmful effects. This is notably the case for pregnant smokers, in whom smoking is one of the main avoidable causes of pregnancy complications, particularly for the newborn child3. In fact, smoking during pregnancy is associated with an excess risk of gestational diabetes, lung infection and extra-uterine pregnancies in women3-5, and with delayed intrauterine growth, central nervous system toxicity, sudden infant death, respiratory problems, and congenital defects in children. Children exposed to smoking are also at increased risk of becoming smokers during their lifetime6-8.
The prevalence of smoking among pregnant women is the highest in the European region9, with about 12.5% in Austria, 16.3% in France and 12–17% in the UK10. Pregnancy, a key event in a woman’s life11, can be considered to be a ‘teachable moment’, i.e. a moment when women are more likely to change their health behaviors12. This period is, therefore, particularly effective for accompanying women in the reduction of tobacco consumption. However, effective smoking cessation strategies applied to the general population appear to have little effect on pregnant women13-15. Therefore, the factors associated with the implementation of strategies remain to be clarified, particularly in this population.
The highly addictive nature of nicotine in tobacco products makes quitting particularly difficult and often requires additional support from a health professional (HP)16. Psychosocial interventions put in place by these professionals appear to be the most recommended for pregnant women, including the 5As model13,17. In pregnant women, the 5As model seems to be effective if the intervention is context sensitive18-22. This model is supported by a high level of evidence23 and aims to identify the smoking status and encourage cessation by proposing strategies adapted to the individual’s degree of motivation24. The 5As method includes five steps: Ask if the woman smokes; Advise her to stop smoking; Assess her motivation, the severity of her addiction and her social environment; Assist to put in place strategies to help her quit smoking; and Arrange follow-up visits throughout the intervention23,24. The 5As model can therefore help coordinate different effective smoking cessation strategies for pregnant women. For example, the ‘Ask’ step can be done using a self-administered questionnaire, the ‘Advise’ step can be done by giving a pamphlet about the benefits of smoking cessation, the ‘Assess’ step can be done using some tools to assess the predictors of smoking cessation, such as the Fagerström test for nicotine dependence25, the ‘Assist’ step can be done prescribing nicotine replacement therapy, and the ‘Arrange’ step can be done using the electronic medical record which can be set to remind the health professional to ask the pregnant women about tobacco.
This type of intervention is complex due to the large number of components involved and the different levels of involvement (e.g. pregnant women, health professionals, local healthcare organizations, and political and legal context)26. The effectiveness of the 5As model in terms of public health depends not only on the five key steps of the intervention but also on the contextual factors in which it is implemented27,28. This article hopes to assist in operationalizing the 5As model within prenatal practice by reviewing studies exploring experiences with pregnant smokers. The objective of this review is to identify the factors that act as barriers or facilitators to the implementation of the 5As model in the health system.
METHODS
A scoping review of the literature following the Arksey and O’Malley methodological framework29 and the PRISMA 2020 statement, which proposes a structured approach with a four-phase flow diagram, and a 27-item checklist30 was conducted (Supplementary file).
Eligibility criteria
Articles were retained if they were in English or French, published between January 2010 and 2021, and concerned pregnant women and the 5As model. We have included all types of settings, quantitative and qualitative research studies, and research designs. Articles detailing the 5As model without mentioning its implementation were excluded. Thus, protocols, guidelines and recommendations were not included.
Information sources and search strategy
In February 2023, we searched PubMed, Scopus and Web of Science, using the terms: ‘smoking cessation’, ‘pregnan*’ and (‘5A’ or ‘5As’) in titles and abstracts.
Selection process and data collection process
The lists of articles found in both databases were manually compared to remove any duplicates. The two reviewers (EC and AB) independently read all the abstracts of the articles found. Articles were excluded if they did not meet the inclusion criteria. Thus, eligible articles were selected on the basis of their abstract by two reviewers (EC and AB) and then were documented in a Microsoft Excel spreadsheet. This document was uploaded on the Bordeaux university hospital’s secure platform, Nextcloud. A kappa statistic was used to measure the correlation between the two reviewers for the abstract screening. Any discrepancies were discussed between the reviewers until a consensus was reached.
The two reviewers then performed a full-text assessment to identify the relevant articles to include in the review. The full articles were analyzed using a grid specifically developed for the study, identifying several elements: authors, title, date, where the study was conducted, and the method used. Three articles were assessed by the two reviewers independently to ensure that they were analyzing the articles in a similar way. During the full-text assessment step, if a study did not meet all of the inclusion criteria, it was excluded. The reviewers then independently identified the factors associated with the implementation of the 5As model present in each study.
Data analysis
The factors identified in the reviews during data extraction were classified by the reviewers into thematic sub-categories and then into thematic categories. These categories and sub-categories were developed inductively, based on the data and specifically for this study. To go further in the classification, we used a theoretical framework from the European Observatory on Health Systems and Policies to organize each of the factors into three levels: a clinical level, an organizational level, and a health systems level31. Thus, the thematic categories of factors have also been classified into the three categories of the theoretical model above.
RESULTS
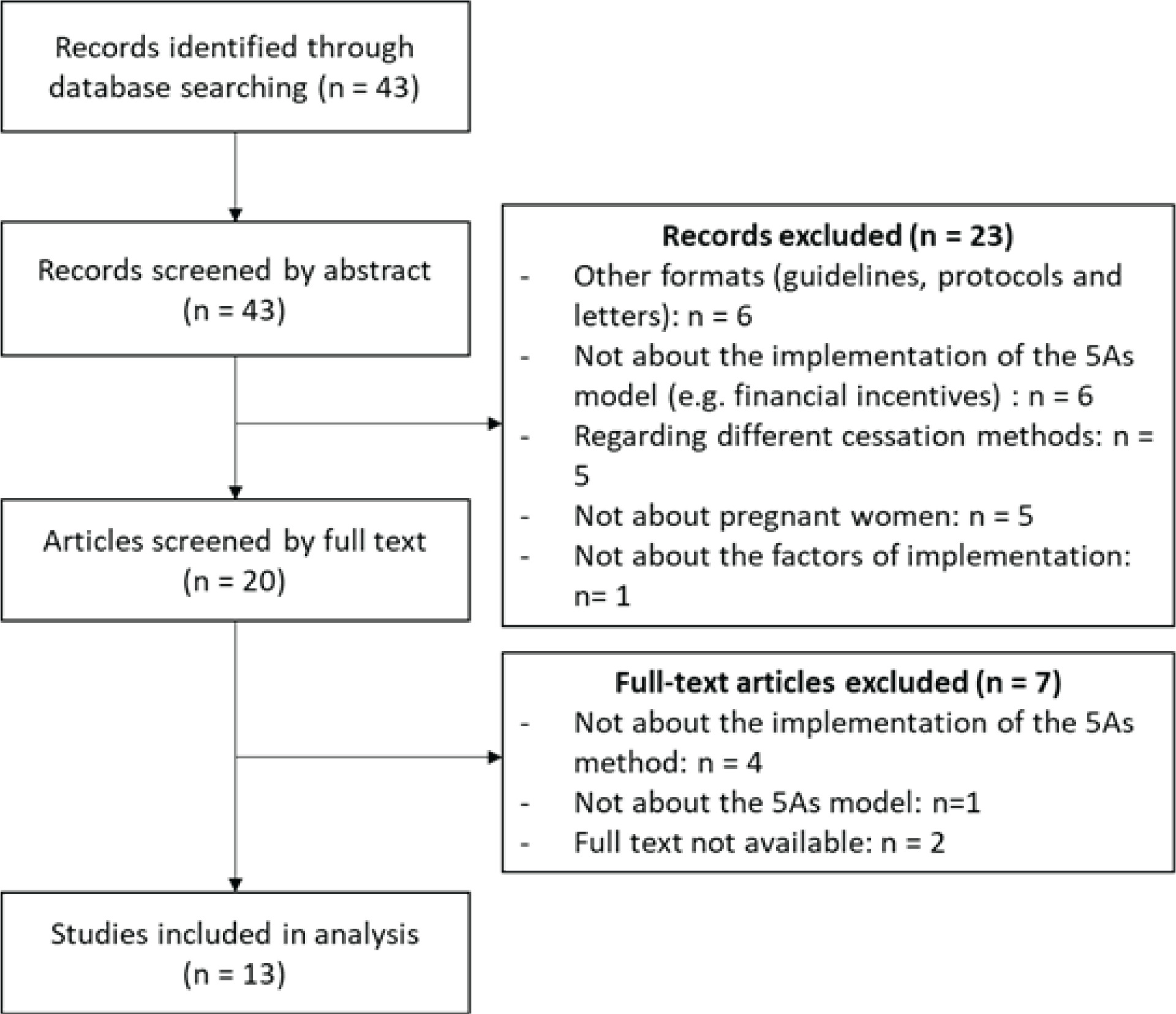
A total of 43 articles were identified. Among them, 13 met the inclusion criteria32-44 (Figure 1). The majority of the articles came from English-speaking countries (Supplementary file Material 1), mainly the USA, Australia and South Africa (n=10; 76.9%). The 5As method is used in many contexts, such as maternal obstetric units, prenatal care clinics, and in the public health system in general.
A thematic analysis of the 13 articles allowed us to identify the factors associated with the implementation of the 5As model. These factors are detailed in the factors associated with the implementation of the 5As model section (Supplementary file Material 2). In total, we identified 48 factors. When necessary, we grouped them together, resulting in 12 sub-categories, which in turn were grouped into 9 categories. The 9 categories are: clinical practices, organization of practices, resources, support for professionals, perceptions of the 5As model, professional role and identity, health professionals’ perceptions of pregnant women, influence of beneficiaries, and the political environment. These 9 categories were then classified into the 3 levels of the theoretical framework described above.
Clinical level
Clinical practices
‘Clinical practices’ refers to the target practices for professionals implementing the 5As model. The category of clinical practices has three sub-categories. Firstly, six studies (46.2%) emphasized the importance of the professional’s approach, attitudes, posture and professional relationship with women in their care34-37,43,44. Similarly, four studies (30.8%) highlighted that interprofessional cooperation as an important element in the successful implementation of the 5As model35-37,41. The last sub-category that was identified by seven studies (53.9%) was the use of practical aids such as motivational interviewing or smoking cessation information materials33-36,38,41,43.
Perceptions of the 5As model
This category takes into account the perceptions of perinatal professionals on the practice of the 5As model. It was not necessary to create subcategories here. Four of the thirteen studies included in this scoping review discussed this theme (30.8%)34,38,40,41.
Professional role and identity
The next category explores the role and identity of perinatal professionals in supporting pregnant women to stop smoking. Three sub-categories were identified. The first is the role perceived by the professionals themselves, which was identified in five studies (38.5%)35,36,40,43,44. The second sub-category is the motivation of these professionals, which also appeared in five studies (38.5%)35,38,39,42,44. Finally, the last sub-category to be considered for the implementation of the 5As model is the self-efficacy of professionals. This was cited by seven studies (53.9%)32,34,35,40,41,43,44.
Health professionals’ perceptions of pregnant women
Another theme that was identified in our thematic analysis was the perceptions that perinatal professionals have of the pregnant smokers for whom they provide care. It may be the professionals’ preconceived notions of pregnant women. This is an element that was mentioned in seven of the thirteen studies in this review (53.9%)34,35,38,39,41,43,44. This category did not require sub-categorization.
Influence of beneficiaries
This theme deals with the influence of the pregnant woman (the beneficiary) on the implementation of the 5As model by perinatal professionals. It was found in three studies (23.1%)35,41,43. There is no subcategory.
Organization level
Organization of practices
These are the organizational factors required for a successful implementation of the 5As model. This second category has two sub-categories which are the organization of the perinatal care pathway, identified in five studies (38.5%)34,35,39,41,44, and the organization of the deployment of the 5As model, also cited by four studies (30.8%)35,36,39,41.
Resources
These are the resources needed to support the implementation of the 5As model. Financial resources and time are the two types of resources mentioned in the literature and therefore constitute the two sub-categories. The issue of financial resources was raised by five studies (38.5%)34,35,37,40,42 and time by eleven studies (84.6%)34-44. Indeed, the majority of the included studies highlighted the lack of time available for professionals in general and during consultations as a barrier to the implementation of the 5As model.
Support for professionals
The next category concerns support for professionals who wish to implement the 5As model with their patients. Here we see that the training of professionals is an important element. Indeed, all the included studies (100%) stressed the importance of training and the acquisition of appropriate skills and knowledge32-44. The second sub-category concerns the resources available to support professionals in the practice of the 5As model. Of the thirteen included studies, six (46.2%) raised the importance of these resources33,35-37,39,41.
DISCUSSION
To the best of our knowledge, this is the first scoping review that focuses on the factors associated with the implementation of the 5As model for pregnant women. Our review identified 49 factors, classified into three different levels: a clinical level, an organizational level, and a health system level. The 5As model is a complex intervention, because ‘of properties of the intervention itself, such as the number of components involved; the range of behaviors targeted; expertise and skills required by those delivering and receiving the intervention; the number of groups, settings, or levels targeted; or the permitted level of flexibility of the intervention or its components’45.
Consequently, several elements must be studied prior to implementation, particularly the contextual elements, since these are in constant interaction with the intervention and are highly influential in the way the intervention is implemented and received. This creates what is known as the ‘interventional system’27 because it takes into account the influence that the environment has on the intervention at the local level28. In the context of the implementation of the 5As model, the environment to be considerate of is the health system, whose functioning changes depending on the region or territory (medical density, territorial organization, etc.). The results of this review highlight the need to take into account the three levels of the interventional system, as they are each influential in the implementation of a 5As intervention31. For example, although the training of professionals is frequently emphasized, it is not the only factor that can be mobilized; the majority of the factors identified in this review are organizational. Therefore, mobilizing several factors at all levels of the interventional system would lead to a more robust implementation of the 5As model46,47.
The complexity of the 5As model does not lie exclusively in the model itself. Indeed, much of this complexity is due to the context in which this model is implemented28. An intervention such as the implementation of the 5As model may be effective in one context but not in another. Adaptation to the context is thus paramount for the intervention to be effective28,47. The factors identified in this review are not context-specific, allowing those interested in implementing the 5As method to identify themselves the factors needed for success in their own environment. This enables the intervention to be flexible and adaptable to different environments and local health system organizations47.
In addition, the nature of the factors identified by this literature review is consistent with pre-existing theoretical frameworks. For example, the theoretical framework proposed by Senn et al.48 also highlights the diversity of domains influencing practice in primary care (patient and population needs, organization and structure of primary care practices, patient and population health outcomes, and delivery of primary care services). The results of this review are consistent with previous studies observing smoking cessation interventions. Indeed, several studies49-51 have demonstrated the importance of individual factors (training, personal experiences, self-efficacy, smoking status, etc.) as well as organizational factors (knowledge/existence of guidelines/resources, organizational support, leadership, etc.) in the implementation of smoking cessation advice by health professionals. Finally, the factors for such a cessation method are numerous and varied. To implement a 5As model intervention, it will be necessary to take into account the many different elements that can influence the intervention.
Strengths and limitations
This study has several strengths and limitations. Some factors may be missing from this report as they have not yet been published for one of several reasons: some experiments of the 5As model may not be documented in written reports, some may be published in the grey literature, and others may be published as indexed articles in non-healthcare databases (e.g. implementation sciences, management sciences). The risk of missing factors is estimated to be low, given the diversity of the selected studies. This diversity ensures that many aspects of the implementation of the 5As model have been explored. Moreover, because of the rigorous method used for this scoping review, we believe we have identified a complete list of the factors that appear in published articles. Furthermore, the databases PubMed, Scopus, and Web of Science were used for this review, which are some of the main reference databases in the health field.
However, it remains impossible to know whether certain factors must be present for the implementation to be effective. While some factors are found every time in the articles and others are found only once, this does not necessarily mean that those that are always present are indispensable and those that are less present are optional. Several conclusions can be drawn from this observation. Further studies are needed in order to determine which factors are truly essential to the implementation of the 5As model. This limitation of our study demonstrates the importance of adapting the intervention to the context by studying what are the specific weaknesses of the environment and how to respond to them.
Finally, because the 5As model is a complex intervention, all the factors identified for a successful 5As intervention are therefore interdependent. This study did not allow us to determine what levels of influence exist between them. For example, we know that the influence of beneficiaries and the support for professionals will have an influence on the perceptions of pregnant women, but we do not know if one has a stronger influence than the other. Further studies exploring these different links are needed to understand the influence pathways and to ensure that all the elements necessary for effective implementation are gathered and prioritized.
Implications
Prior to the implementation, it is necessary to study the factors associated with the implementation of the 5As model in order to adapt to the singularities of each context. Further studies are needed to investigate whether certain factors must be present to guarantee the effectiveness of the implementation or simply have a facilitating role, as well as to identify the chains of influence between the factors.
CONCLUSIONS
There are many factors associated with the implementation of the 5As model, and a selection must be made to ensure effective implementation. Several factors must be taken into account when selecting which to prioritize: the context in which the implementation takes place, the different levels of organization of the health system, and the existing resources. However, further studies are needed to investigate whether certain factors must be present to guarantee the effectiveness of the implementation or simply have a facilitating role, as well as to identify the pathways of influence between the factors.