

INTRODUCTION
Globally 1.3 billion adults use tobacco products and India accounts for 20.5% of current global tobacco use burden1-3. India’s tobacco use landscape is characterized by combustible (cigarettes, and hand-rolled bidis), smokeless (chewing tobacco, ghutka, and khaini etc.) and mixed use (use of combustible and smokeless tobacco)2. Currently, >200 million Indian adults use smokeless tobacco products, and approximately 100 million use combustible tobacco1,2.
India’s tobacco control efforts include bans on advertisements and promotions, demand reduction strategies (such as anti-tobacco advertising campaigns), and provision of tobacco cessation services1. The anti-tobacco advertising campaigns include pictorial health warnings and health education campaigns through various media, including the internet, television, radio, cinema, and other mass media1,4. As a signatory to the World Health Organization (WHO) Framework Convention on Tobacco Control, India has demonstrated strong implementation of Article 14 by 1) mandating quit advice at routine healthcare visits; 2) making nicotine replacement therapy (NRT) and pharmacotherapy (bupropion and varenicline) available; and 3) providing cessation services through over 2000 tobacco cessation centers, government-sponsored mCessation (regular SMS-based support to quit tobacco use), and quitline services1,5.
Despite these interventions, cessation outcomes among people using tobacco in India remain sub-optimal. In 2016–2017, only 14.2% of combustible tobacco users and 6.5% of smokeless tobacco users successfully quit6,7. Further, 36.3% of combustible tobacco users, and 32% of smokeless tobacco users reported past one-year quit attempts, and only 13.4% and 10.9% of quit attempts, respectively, were supported by cessation services6-8. These cessation outcomes are low compared to other countries like Mexico, Brazil, and Russia, and have remained stagnant between 2009 and 20176,9-11. Similar to the United States and European nations12,13, the healthcare provider (HCP) engagement in aiding cessation is limited, with only 51% of tobacco users who visited a HCP receiving advice to quit6,14.
Cessation outcomes are associated with sociodemographic characteristics, tobacco dependence, health status, awareness and attitudes, and social influences. Age, residence, education level, and employment are associated with past quit attempts and successful quitting6,7. Mixed users and individuals with tobacco dependence (i.e. using tobacco within the first 30 minutes of waking) are less likely to quit tobacco use or make quit attempts14,15. Awareness about the negative effects of tobacco use7,15 and poor health status14,15 are both associated with more attempts and higher quit rates. Social influences such as partners’ encouragement to quit tobacco use, exposure to anti-tobacco advertising, and restrictions on smoking at home have a positive impact on cessation behaviors16. Receiving advice to quit from HCP is also associated with quit attempts and successful quitting6,7. Older individuals, those with chronic conditions and combustible tobacco users are more likely to receive HCP quit advice during healthcare visits14.
Tobacco cessation outcomes, including successful quitting, quit attempts, cessation service use, and HCP advice to quit, reflect the successful implementation of broader tobacco control policies1,7,11. However, evidence comprehensively capturing these outcomes for both smoking and smokeless tobacco users in India is scarce. Existing studies assessed cessation behaviors independently among smoking or smokeless tobacco users6-8,14,15, and were primarily based on Global Adult Tobacco Surveys (GATS) and National Family Health Survey (NFHS; 2015–2016), which do not adequately capture the impact of tobacco control interventions such as quitline services, mCessation, and tobacco cessation centers that were expanded after 2016–20171,17. While the Tobacco Control Project (TCP) India Wave 1 (2010–2011) and Wave 2 (2012–2013) surveys captured these data18, latest evidence comprehensively capturing cessation outcomes across various forms of tobacco use in India is lacking. Further, the influence of health status, partner support, tobacco use restrictions, and exposure to broader public health interventions, like anti-tobacco advertising campaigns, on cessation outcomes is less understood.
Using the latest TCP Wave 3 survey (2018–2019)18, we assessed the prevalence of four cessation outcomes: successful quitting, making quit attempts, cessation services use, and receiving HCP advice to quit among exclusive combustible tobacco, exclusive smokeless, and mixed users of both combustible and smokeless tobacco products in India and sought to explore factors associated with these cessation outcomes across these groups. We hypothesized that cessation outcomes would differ by the type of tobacco used, sociodemographic characteristics, health status, and social influences.
METHODS
Study design and study setting
We conducted a secondary analysis of cross-sectional data from the 2018–2019 TCP Wave 3 Survey. The TCP India Survey is part of the International Tobacco Control Policy Evaluation Project (ITC Project) surveys conducted across 31 countries to evaluate the impact of national-level tobacco control policies18. The TCP India Wave 3 Survey is the third round of the recontact and replenishment survey conducted in 2018–2019. Earlier rounds were conducted in 2010–2011 (Wave 1), and 2012–2013 (Wave 2). The TCP India Wave 3 surveyed a total of 10474 participants aged ≥15 years across four states: Bihar, Madhya Pradesh, Maharashtra, and West Bengal. It employed a multi-stage probability sampling approach and used standardized screeners, household and individual survey questionnaires18. The surveys were conducted in participants’ homes by trained field investigators through a manual and computer-assisted personal interviewing approach18.
Study sample and operationalization
In this study, we analyzed a sample of lifetime tobacco users who were exclusive combustible tobacco users (n=977), exclusive smokeless tobacco users (n=5806), and mixed users (n=1157) surveyed at Wave 3. We defined lifetime combustible tobacco use as present or past exclusive use of combustible tobacco products (i.e. cigarettes and/or bidis) at least once a month or smoking 100 or more cigarettes and/or bidis in the lifetime16,18. We defined lifetime smokeless tobacco use as present or past exclusive use of smokeless tobacco products (e.g. gudhaku, gul, ghutka, khaini, mawa, mishri, paan masala with tobacco, plain chewing tobacco etc.) for at least once a month16. Lifetime mixed use was present or past use of both combustible and smokeless tobacco products16,18. We defined current users as those who use combustible and smokeless products daily or less than daily, whether exclusively or in combination. The HCP visits were defined as self-reported visits to a physician or any HCP, within six months before participating in the survey14.
Outcomes
We defined successful quitting as self-reported status of having quit combustible and/or smokeless tobacco at the time of the survey in a lifetime user11. Past quit attempts were defined as any lifetime serious attempt to stop using combustible and/or smokeless tobacco products by a current user9. Cessation service use was defined as the use of approved cessation approaches (i.e. nicotine gum, nicotine patch, bupropion, quitline, counselling, mCessation, cessation clinic) during the latest attempt to quit tobacco use6. We defined HCP advice to quit as receipt of any advice to stop using tobacco products by a HCP within the last six months14. The outcomes were computed specific to the type of tobacco user, and their status of tobacco use. We provide details on how each variable was operationalized in Supplementary file 1.
Covariates
Sociodemographic variables
The sociodemographic variables included: sex (female,male), residence (urban, rural), education level (no formal education, primary and middle school, secondary school, graduate or higher), and employment status (not employed, employed).
Health status
Health status was self-reported as: poor, average, good, and excellent.
Perception that tobacco damaged health
The perception that combustible and/or smokeless tobacco use damaged health was self-reported as: not at all, little damage, and a lot of damage.
Tobacco use dependence
We defined ‘tobacco use dependence’ as the use of combustible or smokeless tobacco products within 30 minutes of waking up19,20.
Awareness about the health effects of tobacco
We computed a composite score (range: 0–24; Cronbach’s alpha=0.93) for awareness about the health effects of smoking (cigarettes/bidi) as a cause for stroke, cancer, heart disease, and other conditions linked with tobacco use. Awareness of health effects of smokeless tobacco products (composite score: 0–6; Cronbach’s alpha=0.85) as cause for stroke, mouth cancer, throat cancer, heart disease, gum disease, and difficulty opening the mouth (Supplementary file 1).
Social influences
We defined partners’ perception of quitting tobacco use based on the responses to items ‘partner thinks you should quit tobacco (smoking/smokeless)’ with the responses ‘No/not applicable’, ‘yes somewhat’, and ‘yes a lot’.
Smoking restrictions at home were self-reported with responses: ‘allowed’, ‘allowed with restrictions’, and ‘not allowed’.
We defined the variable ‘anti-tobacco advertising motivated to quit’ (with responses ‘no/less likely to quit’ and ‘more likely to quit’) based on two items: 1) capturing participant’s exposure to anti-tobacco messages on media (Internet, Television, Cinema etc.); and 2) perception that exposure to anti-tobacco advertising has made them more or less likely to quit (Supplementary file 1).
Analysis
The data cleaning and analysis was conducted using Statistical Package for Social Sciences (SPSS) version 27 [IBM Corp. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp., 2020]. Rescaled cross-sectional weights for the TCP Wave 3 Survey data were applied to account for the complex survey design.
Descriptive statistics (i.e. weighted percentages) were calculated to report prevalence estimates of outcome variables. To examine the association of socioeconomic factors, health dimensions, and social influences with cessation outcomes of successful quitting, past quit attempts, and HCP advice to quit, we conducted binary logistic regression analysis for outcomes across combustible tobacco users and smokeless tobacco users, and multinomial logistic regression analysis for cessation outcomes among mixed users. We developed logistic regression models capturing the main effects and reported adjusted odds ratios (AORs) and 95% confidence intervals (CIs). We identified independent variables for the regression models based on prior literature on tobacco cessation6-8,14-16, and we considered socioeconomic factors as potential confounders. Due to only a few observations, we did not examine factors associated with ‘cessation service use’. We applied sampling weights, to adjust for complex sample design. We assessed multicollinearity using the variance inflation factor (VIF), and a VIF of <2.5 was considered acceptable in our analysis. We used a two-tailed significance level set at α≤0.05.
Ethics approval and informed consent
The 2018–2019 TCP India wave 3 survey was approved by the office of research ethics, University of Waterloo, Canada (ORE#15722) and the Healis Sekhsaria Institute for Public Health International Research Board, India (IRB00007340). Informed consent was obtained from all survey participants. This study was a secondary analysis of de-identified data, which does not meet the definition of human subjects research and therefore did not require review by the Institutional Review Board at the University of California, San Francisco (UCSF).
RESULTS
The majority of participants (n=5806; 73.1%) were smokeless tobacco users, followed by mixed users (use of combustible and smokeless tobacco) (n=1157; 14.6%), and combustible tobacco users (n=977; 12.3%). The majority of lifetime combustible tobacco users and mixed users were males (97.7%, 96.5%), while lifetime smokeless tobacco users had an equal distribution of females (47.2%) and males (52.8%) (Table 1).
Table 1
Cross-sectional analysis of characteristics of lifetime and current tobacco users surveyed in the 2018–2019 TCP India Survey (N=7940)
| Variables | Combustible tobacco users | SLT users | Mixed users | |||
|---|---|---|---|---|---|---|
| Lifetime users (N=977) | Current users (N=881) | Lifetime users (N=5806) | Current users (N=5125) | Lifetime users (N=1157) | Current users (N=604) | |
| Age (years) | % | % | % | % | % | % |
| 15–39 | 29.9 | 31.1 | 38.6 | 38.2 | 33.4 | 42.6 |
| 40–54 | 34.8 | 35.9 | 33.1 | 33.5 | 37.4 | 37.6 |
| ≥55 | 35.2 | 33.0 | 28.3 | 28.2 | 29.2 | 19.8 |
| Sex | ||||||
| Female | 2.3 | 2.4 | 47.2 | 45.3 | 3.5 | 5.0 |
| Male | 97.7 | 97.6 | 52.8 | 54.7 | 96.5 | 95.0 |
| Residence | ||||||
| Urban | 69.2 | 68.9 | 73.3 | 74.3 | 77.8 | 78.1 |
| Rural | 30.8 | 31.1 | 26.7 | 25.7 | 22.2 | 21.9 |
| Education level | ||||||
| No formal education | 18.1 | 13.9 | 26.7 | 26.7 | 16.0 | 19.2 |
| Primary and middle school | 35.3 | 37.1 | 33.1 | 34.0 | 41.5 | 42.4 |
| Secondary school | 29.6 | 24.3 | 29.8 | 29.8 | 31.1 | 27.2 |
| Graduate or higher | 17.0 | 24.8 | 10.3 | 9.5 | 11.3 | 11.2 |
| Employment status | ||||||
| Not employed | 14.7 | 13.9 | 43.9 | 42.1 | 14.4 | 13.1 |
| Employed | 85.3 | 86.1 | 56.1 | 57.9 | 85.6 | 86.9 |
| Health status | ||||||
| Poor | 5.0 | 4.9 | 3.6 | 3.4 | 5.5 | 5.9 |
| Average | 32.3 | 30.9 | 23.6 | 24.8 | 30.2 | 31.9 |
| Good | 51.9 | 53.5 | 47.4 | 48.0 | 49.5 | 50.9 |
| Excellent | 10.8 | 10.6 | 25.4 | 23.7 | 14.7 | 11.3 |
| HCP visit* | ||||||
| No | 68.3 | 70.1 | 75.2 | 75.7 | 71.9 | 74.5 |
| Yes | 31.7 | 29.9 | 24.8 | 24.3 | 28.1 | 25.5 |
| Anti-tobacco advertising motivated to quit | ||||||
| No/less likely to quit | NA | 83.5 | NA | 78.5 | NA | 80.0 |
| More likely to quit | 16.5 | 21.5 | 20.0 | |||
| Awareness, mean (SD)a | 20.2 (5.2) | 20.0 (5.3) | 4.7 (1.8) | 4.7 (1.8) | NA | NA |
| Perceived that tobacco use has damaged health | ||||||
| Not at all | 40.8 | 41.8 | 63.0 | 64.0 | 54.0 | 49.6 |
| Little damage | 23.2 | 21.5 | 29.5 | 29.3 | 20.9 | 18.7 |
| A lot of damage | 35.9 | 36.7 | 7.5 | 6.8 | 25.0 | 31.6 |
| Minutes to first cigarette/bidi after waking | ||||||
| >30 | NA | 44.2 | NA | NA | NA | 64.4 |
| ≤30 | 55.8 | 35.6 | ||||
| Partner thinks you should quit smoking | ||||||
| No/NA | NA | 27.3 | NA | 32.5 | ||
| Yes, somewhat | 18.8 | NA | NA | 16.8 | ||
| Yes, a lot | 53.8 | 50.7 | ||||
| Smoking at home | ||||||
| Allowed | 40.5 | 43.1 | ||||
| Allowed with restrictions | 20.2 | 21.0 | NA | NA | NA | NA |
| Not allowed | 39.3 | 35.9 | ||||
| Minutes to smokeless tobacco use after waking | ||||||
| >30 | NA | NA | NA | 49.0 | NA | 60 |
| ≤30 | 51.0 | 40 | ||||
| Partner thinks you should quit smokeless tobacco | ||||||
| No/NA | NA | 48.5 | NA | 27.4 | ||
| Yes, somewhat | NA | NA | 16.6 | 19.8 | ||
| Yes, a lot | 34.8 | 52.7 | ||||
Prevalence of successful quitting, quit attempts, and HCP advice to quit
The overall prevalence of successful quitting for all tobacco users was 12.4% (95% CI: 11.7–13.1). The prevalence of successful quitting among lifetime users of combustible tobacco (including combustible and mixed users) was 27.7% (95% CI: 25.9–29.5) and among mixed users was 6.3% (95% CI: 5.0–7.6). The prevalence of successful quitting among lifetime users of smokeless tobacco (including smokeless and mixed users) was 12.4% (95% CI: 11.7–13.2) (Figure 1).
Figure 1
Prevalence of cessation outcomes and receipt of healthcare provider advice to quit among tobacco users, 2018–2019 TCP India Survey (N=7940)
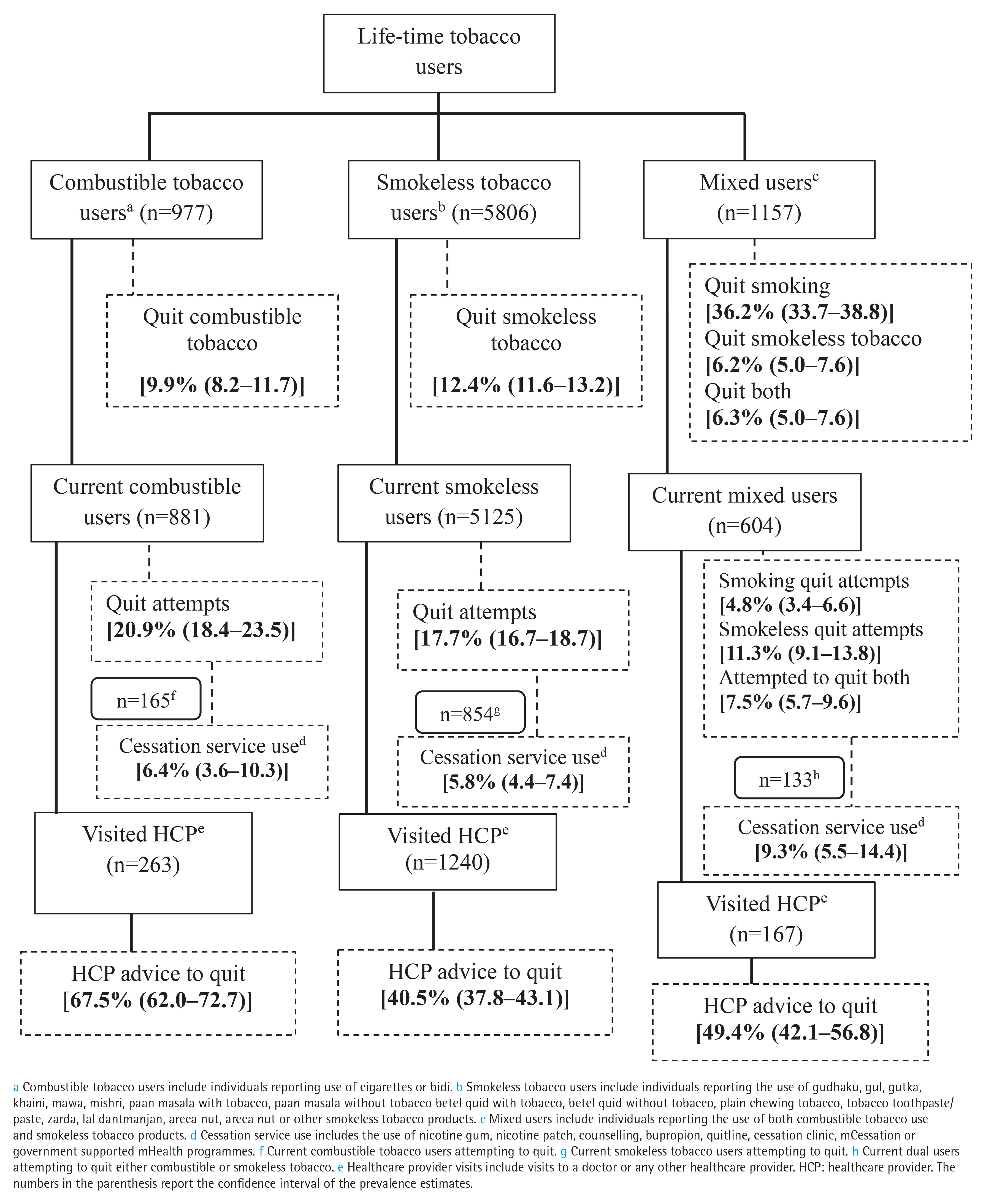
The overall prevalence of quit attempts for current users of any form of tobacco products was 19.7% (95% CI: 18.9–20.6). The prevalence of past quit attempts was 20.9%, 17.7%, and 23.6% for current combustible tobacco users, smokeless tobacco users, and mixed users, respectively while the cessation service use among those attempting to quit was 6.4%, 5.8%, and 9.3% (Figure 1).
Among current users visiting an HCP, combustible tobacco users (n=263) had a higher proportion of receiving quit advice (67.5%) compared to smokeless tobacco users (n=1240) receiving advice to quit (40.5%) and mixed users (n=167) receiving advice to quit either of the tobacco products (49.6%) (Figure 1).
Factors associated with successful quitting, quit attempts, and HCP advice to quit among combustible tobacco users
Successful quitting
Lifetime combustible tobacco users aged ≥55 years (AOR=3.82; 95% CI: 2.06–7.07) compared to individuals aged 15–39 years, individuals with higher awareness scores (AOR=1.14; 95% CI: 1.06–1.22) and living in homes where smoking was not allowed (AOR=5.58; 95% CI: 3.07–10.13) compared to participants reporting ‘smoking was allowed’ in their homes, were more likely to have quit smoking at the time compared to their counterparts (Table 2).
Table 2
Factors associated with cessation behaviors among participants who exclusively use combustible or smokeless tobacco during the 2018–2019 TCP India Survey
| Independent variables | Combustible tobacco a | Smokeless tobacco b | ||||
|---|---|---|---|---|---|---|
| Successfully quit (N=977) | Quit attempts c (N=881) | Healthcare provider advice to quit (N=263) | Successfully quit (N=5806) | Quit attempts c (N=5125) | Healthcare provider advice to quit (N=1240) | |
| AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | |
| Age (years) | ||||||
| 15–39 ® | ||||||
| 40–54 | 1.36 (0.71–2.61) | 1.14 (0.72–1.82) | 1.24 (0.53–2.87) | 0.89 (0.73–1.08) | 1.25 (1.04–1.50)* | 0.93 (0.66–1.30) |
| ≥55 | 3.82 (2.06–7.07)** | 1.15 (0.70–1.87) | 1.59 (0.71–3.58) | 1.07 (0.86–1.33) | 1.05 (0.85–1.29) | 1.38 (0.97–1.95) |
| Sex | ||||||
| Female ® | ||||||
| Male | 0.51 (0.11–2.43) | 4.48 (0.50–40.41) | 5.09 (0.53–48.89) | 0.46 (0.37–0.58)** | 0.66 (0.53–0.82)** | 1.01 (0.73–1.40) |
| Residence | ||||||
| Urban ® | ||||||
| Rural | 1.28 (0.75–2.18) | 0.81 (0.52–1.26) | 1.38 (0.64–2.97) | 1.50 (1.26–1.80)** | 0.48 (0.39–0.58)** | 1.06 (0.78–1.43) |
| Education level | ||||||
| No formal education ® | ||||||
| Primary and middle school | 1.18 (0.52–2.72) | 1.91 (1.03–3.54)* | 0.95 (0.38–2.33) | 0.98 (0.78–1.24) | 1.32 (1.07–1.64)* | 0.46 (0.34–0.63)** |
| Secondary school | 1.93 (0.83–4.49) | 2.84 (1.48–5.47)** | 0.51 (0.20–1.32) | 1.42 (1.12–1.81)** | 1.37 (1.09–1.73)** | 0.41 (0.28–0.59)** |
| Graduate or higher | 2.28 (0.93–5.60) | 3.18 (1.54–6.56)** | 0.91 (0.32–2.60) | 2.59 (1.92–3.50)** | 0.87 (0.61–1.23) | 0.42 (0.24–0.74)** |
| Employment status | ||||||
| Not employed ® | ||||||
| Employed | 0.64 (0.35–1.18) | 0.87 (0.50–1.52) | 0.94 (0.40–2.20) | 0.81 (0.66–0.99)* | 1.47 (1.19–1.81)** | 1.21 (0.89–1.64) |
| Tobacco use dependenced | ||||||
| No ® | ||||||
| Yes | NA | 1.50 (1.01–2.24)* | 1.26 (0.66–2.43) | NA | 1.21 (1.04–1.42)* | 1.31 (1.02–1.69)* |
| Perceived that tobacco use has damaged healthe | ||||||
| Not at all ® | ||||||
| Little damage | 2.15 (1.24–3.73)** | 2.90 (1.80–4.67)** | 4.10 (1.56–10.79)** | 1.33 (1.11–1.60)** | 0.89 (0.75–1.06) | 1.91 (1.45–2.52)** |
| A lot of damage | 0.77 (0.44–1.37) | 1.23 (0.79–1.90) | 3.76 (1.84–7.70)** | 2.35 (1.79–3.08)** | 1.06 (0.79–1.42) | 1.53 (0.98–2.40) |
| Awareness, mean (SD)f | 1.14 (1.06–1.22)** | 1.01 (0.97–1.05) | 1.00 (0.94–1.06) | 1.01 (0.97–1.07) | 1.11 (1.06–1.17) | 1.11 (1.04–1.19) |
| Anti-tobacco advertising motivated to quit | ||||||
| No difference/less likely to quit ® | ||||||
| More likely to quit | NA | 2.13 (1.37–3.33)** | 0.97 (0.44–2.12) | NA | 1.82 (1.53–2.16)** | 1.39 (1.04–1.86)* |
| Partner thinks you should quit tobacco useg | ||||||
| No/NA ® | ||||||
| Yes, somewhat | NA | 0.66 (0.33–1.31) | 0.56 (0.22–1.44) | NA | 1.05 (0.82–1.34) | 0.95 (0.65–1.39) |
| Yes a lot | 1.97 (1.23–3.15)** | 0.53 (0.24–1.20) | 2.21 (1.85–2.64)** | 1.77 (1.30–2.42)** | ||
| Smoking at home | ||||||
| Allowed ® | ||||||
| Allowed with restrictions | 1.65 (0.78–3.51) | 0.56 (0.32–0.99)* | 2.17 (0.91–5.17) | |||
| Not allowed | 5.58 (3.07–10.12)** | 2.19 (1.43–3.35)** | 1.07 (0.53–2.17) | NA | NA | NA |
| Health status | ||||||
| Poor ® Average | 2.77 (0.92–8.35) | 0.49 (0.22–1.11) | 0.45 (0.13–1.53) | 0.57 (0.37–0.88)* | 0.75 (0.50–1.13) | 0.74 (0.48–1.14) |
| Good | 1.47 (0.49–4.45) | 0.42 (0.19–0.94)* | 0.56 (0.16–1.98) | 0.85 (0.56–1.29) | 0.58 (0.39–0.87)** | 0.58 (0.37–0.90)* |
| Excellent | 2.92 (0.84–5.60) | 0.32 (1.54–6.56)* | 1.27 (0.26–6.28) | 1.40 (0.91–2.15) | 0.48 (0.31–0.74)** | 0.37 (0.21–0.66)** |
| Received quit advice from healthcare provider | ||||||
| No/NA ® | ||||||
| Yes | 1.19 (0.69–2.05) | 1.77 (1.12–2.79)* | NA | 0.88 (0.65–1.19) | 2.07 (1.65–2.59)** | NA |
b Smokeless tobacco users include individuals reporting the use of gudhaku, gul, gutka, khaini, mawa, mishri, paan masala with tobacco, paan masala without tobacco betel quid with tobacco, betel quid without tobacco, plain chewing tobacco, tobacco toothpaste/paste, zarda, lal dantmanjan, areca nut or other smokeless tobacco products.
c Quit attempts are defined as any serious attempts to stop smoking by a tobacco user reporting the use of tobacco products at least less than once a month.
d Tobacco use dependence was defined as time to use smoking/smokeless tobacco products within 30 minutes of waking.
f Awareness was computed as a composite index of 24 items capturing the awareness about health effects of cigarettes and bidis (composite score of 0-24) for combustible tobacco users; and six items (composite score of 0-6) for smokeless tobacco users.
g Spouse/partner thinks that the respondent should quit smoking/smokeless tobacco products. The multivariable analysis was conducted employing binary logistic regression analysis. ® Reference categories. TCP: Tobacco Control Policy India Survey. AOR: adjusted odds ratio. NA: not applicable. The variables: 1) tobacco use dependence, 2) anti-tobacco advertising motivated to quit, and 3) partner thinks you should quit tobacco use were not measured among participants who successfully quit tobacco use as they were captured only among the current users; ‘Smoking at home’ was not included for the models capturing cessation outcomes across exclusive smokeless users.
Quit attempts
Among current users, individuals with education level of graduate or higher (AOR=3.18; 95% CI: 1.54–6.56) compared to those with no formal education, reporting ‘partner thinks they should quit smoking’ (AOR=1.97; 95% CI: 1.23–3.15) compared to those reporting no/not applicable, and receiving HCP advice to quit (AOR=1.77; 95% CI: 1.12–2.79) compared to those who did not receive it, had higher odds of quit attempts (Table 2).
HCP advice to quit
Among individuals visiting HCP, reporting tobacco use had caused ‘a lot of damage to health’ had greater odds of receiving advice to quit (AOR=3.76; 95% CI: 1.84–7.70) when compared to combustible tobacco users who reported that smoking has ‘not at all’ damaged their health (Table 2).
Factors associated with successful quitting, quit attempts, and HCP advice to quit among smokeless tobacco users
Successful quitting
Males (AOR=0.46; 95% CI: 0.37–0.82) compared to females, and those reporting an average health status (AOR=0.57; 95% CI: 0.37–0.88) compared to individuals reporting a poor health status were less likely to quit smokeless tobacco (Table 2).
Quit attempts
Participants aged 40–54 years (AOR=1.25; 95% CI: 1.04–1.50) compared to those aged 15–39 years, reporting anti-tobacco advertising made them more-likely to quit (AOR=1.82; 95% CI: 1.53–2.16), and reporting receiving HCP advice to quit (AOR=2.07; 95% CI: 1.65–2.59) compared to not receiving one, were more likely to make quit attempts (Table 2).
HCP advice to quit
Among those visiting an HCP, individuals reporting excellent health (AOR=0.37; 95% CI: 0.21–0.66) compared to those reporting poor health, had lower odds of receiving advice to quit (Table 2).
Factors associated with successful quitting, quit attempts, and HCP advice to quit among mixed users
Successful quitting
Mixed users aged ≥55 years had higher odds of quitting both smokeless and combustible tobacco (AOR=7.14; 95% CI: 3.33–15.31) compared to those in aged 15–39 years. A perception that tobacco use had caused ‘a lot of damage to health’ was associated with higher odds of quitting both products (AOR=3.90; 95% CI: 2.07–7.34) compared to those perceiving tobacco use has ‘not at all damaged health’ (Table 3).
Table 3
Factors associated with cessation behaviors among mixed users surveyed in the 2018–2019 TCP India Survey (N=1157)
| Independent variables | Lifetime mixed users | ||
|---|---|---|---|
| Successfully quit smokeless tobacco | Successfully quit combustible tobacco | Successfully quit both | |
| AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | |
| Age (years) | |||
| 15–39 ® | |||
| 40–54 | 1.94 (1.02–3.68)* | 1.89 (1.38–2.61)** | 0.83 (1.36–5.90)** |
| ≥55 | 4.90 (2.51–9.57)** | 4.42 (3.05–6.40)** | 7.14 (3.33–15.31)** |
| Sex | |||
| Female ® | |||
| Male | 2.59 (0.32–21.01) | 2.46 (1.07–5.63)* | 1.45 (0.28–7.66) |
| Residence | |||
| Urban ® | |||
| Rural | 1.01 (0.57–1.81) | 0.89 (0.64–1.24) | 1.95 (1.08–3.54)* |
| Education level | |||
| No formal education ® | |||
| Primary and middle school | 1.69 (0.84–3.40) | 1.50 (1.01–2.25)* | 4.42 (1.44–13.57)** |
| Secondary school | 1.18 (0.53–2.63) | 2.36 (1.55–3.61)** | 9.65 (3.12–29.91)** |
| Graduate or higher | 1.76 (0.69–4.46) | 1.52 (0.88–2.60) | 8.76 (2.55–30.03)** |
| Employment status | |||
| Not employed ® | |||
| Employed | 2.76 (1.08–7.06)* | 0.95 (0.62–1.45) | 0.57 (0.28–1.17) |
| Perceived that tobacco has damaged health | |||
| Not at all ® | |||
| Little damage | 1.04 (0.53–2.03) | 0.95 (0.69–1.32) | 2.04 (0.93–4.46) |
| A lot of damage | 1.18 (0.68–2.05) | 0.16 (0.11–0.25)** | 3.90 (2.07–7.34)** |
| Health status | |||
| Poor ® | |||
| Average | 0.67 (0.25–1.78) | 1.02 (0.53–1.95) | 0.90 (0.24–3.30) |
| Good | 0.81 (0.31–2.12) | 1.03 (0.54–1.96) | 1.93 (0.54–6.90) |
| Excellent | 0.43 (0.11–1.63) | 2.09 (1.03–4.24)* | 4.95 (1.29–18.93)* |
| Received healthcare provider advice to quit | |||
| No/NA ® | |||
| Yes | 1.59 (0.84–3.00) | 1.18 (0.78–1.78) | 1.22 (0.59–2.53) |
Quit attempts
The mixed users reporting anti-tobacco advertisements motivated them to quit had quit combustible tobacco (AOR=4.49; 95% CI: 1.94–11.30), smokeless tobacco (AOR=2.20; 95% CI: 1.20–.04), and both combustible and smokeless tobacco (AOR=3.36; 95% CI: 1.66–6.78) compared to the mixed users reporting no difference/ less likely to quit (Table 4).
Table 4
Factors associated with quit attempts and healthcare provider advice to quit among mixed users surveyed in 2018–2019 TCP India Survey (N=604)
| Independent variables | Current mixed users (N=604) a | Visited HCP (N=167) b | ||
|---|---|---|---|---|
| Attempted to quit combustible tobacco use | Attempted to quit smokeless tobacco use | Attempted to quit both | Received HCP advice to quit | |
| AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | |
| Age (years) | ||||
| 15–39 ® | ||||
| 40–54 | 1.06 (0.41–2.75) | 0.55 (0.30–1.00) | 1.05 (0.50–2.22) | 0.74 (0.32–1.69) |
| ≥55 | 1.25 (0.37–2.75) | 0.59 (0.26–1.31) | 2.13 (0.86–5.27) | 0.88 (0.30–2.56) |
| Sex | ||||
| Female ® | ||||
| Male | 2.00 (0.11–35.39) | 0.27 (0.11–0.71)** | 1.19 (0.14–10.00) | 3.83 (0.42–35.07) |
| Residence | ||||
| Urban ® | ||||
| Rural | 0.44 (0.13–1.49) | 1.08 (0.57–2.04) | 0.16 (0.04–0.61)** | 1.08 (0.45–2.59) |
| Education level | ||||
| No formal education ® | ||||
| Primary and middle school | 2.42 (0.63–9.23) | 0.70 (0.34–1.43) | 1.71 (0.62–4.69) | 1.14 (0.45–2.87) |
| Secondary school | 1.68 (0.40–7.14) | 0.98 (0.46–2.08) | 1.03 (0.33–3.18) | 2.36 (0.82–6.81) |
| Graduate or higher | 0.88 (0.12–6.40) | 0.60 (0.20–1.86) | 2.26 (0.69–7.38) | 1.64 (0.37–7.23) |
| Employment status | ||||
| Not employed ® | ||||
| Employed | 0.78 (0.21–2.89) | 1.05 (0.45–2.45) | 2.79 (0.83–9.37) | 0.95 (0.32–2.83) |
| Anti-tobacco advertising motivated to quit | ||||
| No difference/less likely to quit ® | ||||
| More likely to quit | 4.69 (1.94–11.30)** | 2.20 (1.20–4.04)** | 3.36 (1.66–6.78)** | 0.85 (0.36–1.98) |
| Health status | ||||
| Poor ® | ||||
| Average | 0.11 (0.06–2.12) | 0.41 (0.14–1.25) | 0.16 (0.05–0.52)** | 1.81 (0.64–5.13) |
| Good | 0.67 (0.16–2.88) | 0.37 (0.12–1.11) | 0.29 (0.09–0.92)* | 0.76 (0.26–2.24) |
| Excellent | 0.32 (0.07–1.47) | 0.31 (0.08–1.20) | 0.08 (0.01–0.48)** | 0.68 (0.13–3.59) |
| Received HCP advice to quit | ||||
| No/NA ® | ||||
| Yes | 1.56 (0.54–4.53) | 2.02 (0.96–4.26) | 2.00 (0.85–4.75) | NA |
| Perceived that tobacco has damaged health | ||||
| No damage ® | ||||
| Little damage | 0.60 (0.10–3.50) | 0.66 (0.32–1.37) | 0.60 (0.20–1.76) | 1.11 (0.36–3.42) |
| A lot of damage | 4.23 (1.61–11.16)** | 0.54 (0.28–1.07) | 1.29 (0.63–2.64) | 2.47 (1.16–5.29)* |
HCP advice to quit
Mixed users reporting that tobacco use caused ‘a lot of damage to health’ were more likely to receive advice to quit from an HCP during the latest visit (AOR=2.47; 95% CI: 1.16–5.29) compared to those reporting no damage (Table 4).
DISCUSSION
In this sample of tobacco users in India, individuals with a history of combustible tobacco use were more likely to quit, attempt to quit, use cessation services, and receive HCP advice to quit compared to smokeless tobacco users. Overall prevalence of quitting smoking among all combustible users was consistent with previous estimates11. The overall prevalence of quitting smokeless tobacco was higher than the smokeless tobacco quit prevalence of 8.7%–6.6% reported earlier6,21, and consistent with the declining trend of smokeless tobacco use in India22,23. Our study adds to the literature by providing quit rates disaggregated by tobacco use, and by showing that successful quitting is concentrated among mixed users.
Our estimates of quit attempts of 19.7% across all current tobacco users were lower than the 25% observed in the first wave of TCP survey (2010–2011) in India16. The decline is driven by the stagnation in quit attempts among combustible tobacco users (36.2% in 2009 and 36.4% in 2016), and smokeless tobacco users (33.7% in 2009 and 32% in 2016) observed previously11,15.
Consistent with previous studies, less than one in ten tobacco users used cessation services in their latest quit attempt5,6,15. The low use of cessation services could be due to: 1) fewer people attempting to quit, 2) lack of awareness, and 3) low density of available cessation support services5,17. Furthermore, the limited engagement of HCPs in providing quit advice cannot be ignored. Our estimates indicate combustible tobacco users were more likely to receive advice to quit14,24. while more than half of smokeless tobacco and mixed users are missed possibly due to lack of preparation of HCPs to intervene24, the social context of smokeless tobacco use, and perceived harmlessness of smokeless tobacco products25,26.
Previous studies reported that individuals aged ≥45 years are more likely to quit tobacco use6,7. Our estimates indicate a higher probability of quitting all forms of tobacco use in the older years (aged ≥55 years), contradicting the international evidence, which reports that older people find it harder to quit tobacco use27. In India, quit attempts are more prevalent among younger population, while older populations are more likely to successfully quit6,7. Although access to cessation support is equally limited, older individuals, owing to their health status, may be more inclined to attempt to quit, interact with a HCP, and receive advice to quit tobacco use from an HCP6,7,14. This also aligns with our findings, where individuals reporting that tobacco use caused ‘a little damage’ or ‘a lot of damage’ to their health were more likely to quit tobacco use compared to those reporting ‘no damage’. Our findings add to the evidence on the positive role of HCP advice to quit in improving quit attempts6-8.
Consistent with earlier studies, we found a higher probability of attempting to quit tobacco use among females, individuals with better education, and poor health status14,16. Among the mixed users, higher levels of education were associated with quitting smoking but not smokeless tobacco use6. Most mixed users reported quitting smoking but continued to use smokeless tobacco15. Similar to studies in the United States and China, we also found that partners’ support to quit tobacco use was associated with making quit attempts28,29 and combustible tobacco users living in homes where smoking is not allowed were more likely to quit smoking30. Qualitative studies in India have shown family is a powerful motivator to quit tobacco use25,31. However, further research is required to investigate the role of spousal support in tobacco cessation in the Indian context.
Anti-tobacco messaging campaigns that include messages on tobacco packages, public places, workplaces, and mass media have been shown to be associated with intention to quit and quit attempts4,16. However, <25% tobacco users perceived that the anti-tobacco advertising made them more likely to quit tobacco use, and not everyone was equally exposed to effective anti-tobacco campaigns4. This indicates the need to improve the quality, content, and acceptability of the anti-tobacco campaigns4, while simultaneously ensuring the provision of cessation services.
Strengths and limitations
The study’s strength is its use of the latest wave of the TCP survey, and a comprehensive outlook to cessation outcomes across combustible, smokeless, and mixed users. The limitations include the use of self-reported items with a potential for recall, misclassification, and social desirability bias. Findings may not be generalizable beyond the four states where data collection took place or to other countries. We are unable to infer causal associations with a cross-sectional study design, and there may be a potential for residual unmeasured confounding even as we adjusted for known confounders. Despite these limitations, the study offers the latest estimates for tobacco use cessation in India, providing valuable insights to strengthen the country’s tobacco control efforts.
CONCLUSIONS
In India, one in ten lifetime tobacco users successfully quit, while one in five current users attempted to quit, and less than one in ten tobacco quit attempts was supported by cessation services. The findings indicate the need to strengthen comprehensive tobacco control strategies and support cessation. Anti-tobacco advertising campaigns, tobacco use restrictions in home, spousal support and healthcare provider engagement could be crucial to improve cessation outcomes, and warrant further exploration in longitudinal cessation studies.