

INTRODUCTION
Bone healing occurs following a bone fracture. As described by ElHawary et al.1, this process is categorized as either primary or secondary bone healing. Primary bone healing occurs when the distal and proximal bone fragments are perfectly reduced and aligned under compression1.
Secondary bone healing is a more common process in which the bone heals indirectly in a four-stage process: formation of hematoma, fibrocartilaginous callus, and bony callus, followed by bone remodeling1.
If the process of bone healing takes >12 weeks, it is defined as a delayed union fracture2. Furthermore, in the absence of radiological signs of bone healing for 10 weeks post-injury, the fracture is classified as a nonunion fracture3. However, if bone healing occurs and the bone heals in an abnormal position, the term malunion is used to describe the fracture3.
These impairments in bone healing increase the duration of hospital stay and treatment costs. Fracture-healing complications were the cause of re-admission in 8.1% of patients treated for bone fractures in a study of 3886 patients and these re-admissions accounted to $4.9 million Australian Dollars4. Moreover, the cost of treating a long bone nonunion averaged $11800, US$11333, and £29204 in Canada, the USA, and the UK, respectively5.
Cigarette smoking negatively affects bone healing. Through vasoconstriction, nicotine decreases blood perfusion to target tissues, such as muscles, tendons, ligaments, and bones, thereby impairing bone healing6. A 2022 study found that cigarette smoking increased the risk of fracture nonunion by 91% in spine surgeries and 104% in autograft recipients7. According to a study conducted in Riyadh by Aldhafian et al.4, smoking was the most common patient-dependent risk factor associated with fracture-healing failure. This effect appears to apply to e-cigarettes as well; one study showed that e-cigarette users have a 46% higher prevalence of self-reported fragility fractures8.
According to the Global Adult Tobacco Survey, 17.9% of the Saudi population are smokers, with a prevalence of 27.5% among men and 3.5% among women9. A 2019 study found that the prevalence of tobacco smoking among Saudi university students was 17%10. The World Health Organization states that 22.3% of the global population uses tobacco11.
Smoking exerts harmful effects on bone health. It increases the risk of osteoporosis and delays bone healing in fracture settings12,13. Various studies have highlighted the need to raise public awareness of its risks14,15.
Studies on the Saudi population’s perceptions of the effects of smoking on fracture healing are lacking, which are important considering the burden of delayed fracture healing due to the high prevalence of smoking. To address this issue, our study aimed to provide local original data to build a more comprehensive understanding of the population’s knowledge on the effects of smoking on fracture healing. Access to such data will facilitate the filling of patient knowledge gaps by healthcare providers.
METHODS
Data, study population, and variables
This cross-sectional study was conducted between June and September 2024 in Saudi Arabia. Saudi individuals aged ≥18 years were included in this study. A total of 1033 participants filled in the questionnaires electronically via social media platforms.
The questionnaire consisted of 32 questions divided into three sections. The first part comprised sociodemographic data. The second part included our validated and reliable Smoking and Fractures Knowledge Assessment Tool (SFKAT) (Supplementary file Appendix 1). This tool consists of ten questions. Each question can be answered by ‘true’, ‘not sure’, or ‘false’. A correct answer is calculated as two points, ‘not sure’ is calculated as one point, and an incorrect answer is calculated as zero points. The maximum total score is 20 points. The median score was used to classify the participants into good- and poor-knowledge groups, with participants receiving scores at or above the median classified into the good-knowledge group. The third section of the questionnaire aimed to obtain information on the primary sources of knowledge that the participants used to learn about smoking and fractures. This approach was implemented in a study by Alshammari et al.16. Forward and back-translations were used to translate the survey. We then conducted a pilot study with 45 participants and added open-ended questions at the end of each section to assess the simplicity and clarity of each part and correct any misunderstandings. The questionnaire was then distributed through social media platforms to the participants using snowball sampling.
A priori sample-size calculations and justifications were based on two approaches. G*Power was used for the binary logistic regression (Wald test). We assumed a medium effect size (OR=1.5), α=0.05, power=0.80, and R2=0.1. This resulted in a minimum sample size of 231 participants, which was required to detect a significant association for a single predictor. The 10 events per variable rule was then applied to confirm the stability of the multivariable binary logistic regression model. With 14 predictors and 549 participants classified as having ‘good knowledge’, the final sample of 1033 participants exceeded both criteria, supporting the adequacy of the sample size for a robust analysis.
Validity and reliability of the SFKAT
A specialist in orthopedic surgery confirmed that the questions were clear and accurate and that they aligned with our primary objective. The tool showed excellent internal consistency, with a split-half reliability of 0.87 and a Spearman-Brown coefficient of 0.93. Confirmatory factor analysis showed moderate construct validity with acceptable model fit indices (comparative fit index=0.92, Tucker-Lewis index=0.9, and root mean square error of approximation=0.099). Five of ten items of the SFKAT had factor loadings exceeding 0.4, indicating partial structural validity. These results suggest that the SFKAT is a moderately valid and highly reliable instrument to assess knowledge in this population.
Ethics
The study was approved on 10 June 2024, by the Institutional Review Board of the King Saud University with reference number E-24-8893. Consent was obtained from all participants before they completed the questionnaire. The respondents’ anonymity was maintained. The data were used exclusively for research purposes.
Statistical analysis
IBM SPSS Statistics software for Windows (version 21.0; IBM Corp., Armonk, N.Y., USA) was used to analyze the data. Categorical variables are described using descriptive statistics (frequency and percentage). Continuous variables are described using median and interquartile range (IQR). The relationship between categorical study variables and outcome variables was analyzed using Pearson’s chi-squared test. ORs were used as indicators of the association between two categorical variables. For multivariate analysis, a binary logistic regression model was implemented to identify the independent predictors of knowledge levels. The process of variable selection in the model was based on a combination of statistical significance and theoretical relevance. Variables with a p<0.2 in the univariate analysis were included. Age and sex were included a priori because of their known influence on health-related knowledge. Nineteen variables were included in the final model. Adjusted ORs (AORs) with 95% confidence intervals (CIs) are reported. Model fit was tested using the Hosmer-Lemeshow goodness-of-fit test. Explanatory power was evaluated using Cox and Snell R2 and Nagelkerke R2 statistics. The analyzed data are displayed using tabular and graphical presentation methods. The study reported data precision through 95% CIs and statistical significance levels at p<0.05. To assess the robustness of the median-based knowledge classification, a sensitivity analysis was conducted using alternative cut-off values: the upper 33rd percentile (score ≥18) and the upper 25th percentile (score ≥19). Binary logistic regression was repeated using these alternative definitions of ‘good knowledge’, and model consistency was compared.
RESULTS
Sociodemographic characteristics and descriptive statistics
The total sample consisted of 1033 participants aged 18–85 years. Age distribution was positively skewed, with a median age of 39 years (IQR=25–50). Among the participants, 54.4% were men. In addition, 29% of participants reported a history of fractures. Among the sample, 249 participants (24.1%) reported smoking behaviors, including cigarettes, vaping, or shisha (Supplementary file Appendix 2). Approximately 87% of smokers were men. The prevalence of smoking was 38.4% in men and 7% in women. In addition, 61% of the smokers were aged 26–50 years.
Descriptive statistics of the total scores
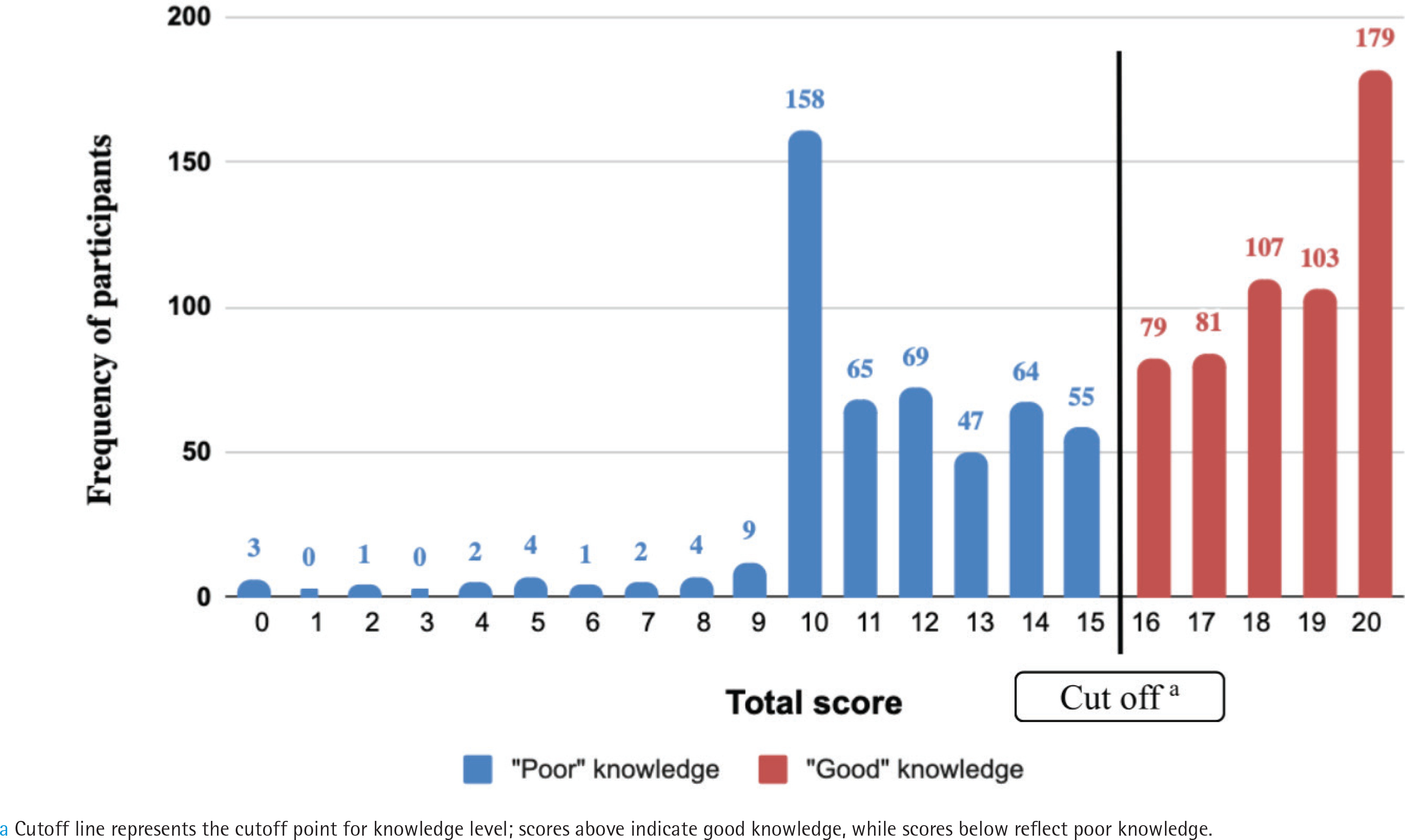
The total scores obtained from the SFKAT followed a non-parametric negatively skewed distribution (Figure 1), with a median of 16 (IQR=12–19). Almost 53% of participants had good levels of knowledge. Female participants had a median total score of 17 (IQR=14–19). Most of the women had a good level of knowledge (64.5%). For men, the median total score was 14 (IQR=10–18), with only 43.6% scoring a good level of knowledge. The median total score of smokers was 13 (IQR=10–17), whereas that of non-smokers was 17 (IQR=12–19). Only 35% of smokers scored a good-knowledge level compared with 59% of non-smokers.
Main sources of knowledge
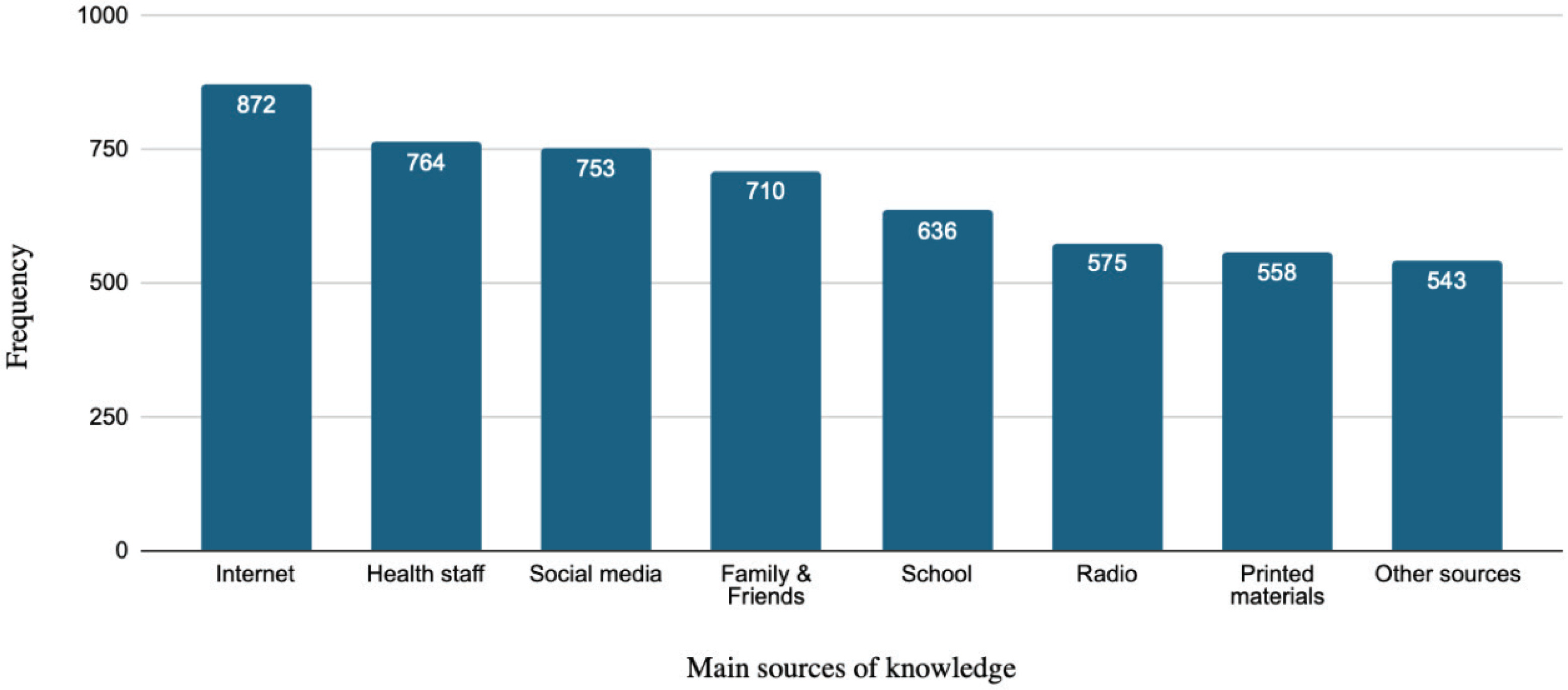
Regarding knowledge acquisition, participants relied predominantly on the internet (84%) and healthcare personnel (74%) as their main sources of information. The least common sources included radio, printed materials, and ‘other sources’ (Figure 2).
Association between sociodemographic characteristics and level of knowledge
The odds of having a good level of knowledge were lower in men than in women (OR=0.43; 95% CI: 0.33–0.55; p<0.001). The odds of having a good level of knowledge were 2.29 times greater among participants working in healthcare fields than those in non-health professions (95% CI: 1.66–3.17; p<0.001). The participants with a history of fracture had 29% lower odds of acquiring a good level of knowledge compared to those who did not have a fracture history (95% CI: 0.55–0.93; p=0.014). Regarding smoking status, the analysis reported smoking cigarettes, shisha, or vaping was associated with a lower likelihood of having a good level of knowledge compared to non-smokers (OR=0.38; 95% CI: 0.29–0.52; p<0.001) (Table 1).
Table 1
Association between the dichotomous sociodemographic characteristics and the level of knowledge of the Saudi population, a cross-sectional study conducted in Saudi Arabia, June–September 2024 (N=1033)
Age groups were significantly related to the level of knowledge, as the respondents who had a good level of knowledge in those aged ≥51 years, were significantly lower than the expected count of respondents, while all other age groups had higher counts than expected (p=0.048). No significant association was noted between the level of knowledge and any other polytomous demographic variables.
Association between main sources and level of knowledge
Using the internet as a primary source of knowledge was not significantly related to the level of knowledge. However, all remaining sources had a statistically significant association with the level of knowledge, with varying ORs (Table 2). Participants who chose school as their source of information were 1.03 times more likely to have a good level of knowledge. Additionally, participants who sought healthcare personnel as knowledge source were 1.83 times more likely to have a good level of knowledge. Participants who utilized ‘other sources’ to gain knowledge had the highest likelihood of having a good level of knowledge (OR=2.04).
Table 2
Association between the main sources of knowledge and the level of knowledge of the Saudi population, a cross-sectional study conducted in Saudi Arabia, June–September 2024 (N=1033)
Binary logistic regression analysis of variables significantly associated with the level of knowledge
Multivariable binary logistic regression analysis revealed that sex; working in the healthcare field; smoking cigarettes, shisha, or vape; and ‘other sources’ were independently associated with the knowledge level, after adjusting for potential confounders. These associations persisted after adjustments, suggesting that they were not fully explained by the included confounders (Table 3). Men were 0.48 times less likely to achieve a good level of knowledge (95% CI: 0.36–0.65; p<0.001). Healthcare workers had a higher likelihood of achieving good level of knowledge (AOR=2.78; 95% CI: 1.90–4.08; p<0.001). Smokers had lower odds of scoring a good knowledge level than non-smokers (AOR=0.54; 95% CI: 0.38–0.75; p<0.001). The multivariable logistic regression model demonstrated good calibration, as indicated by the non-significant Hosmer-Lemeshow test (p=0.614). The model explained approximately 19.1% of the variance in knowledge levels (Nagelkerke R2=0.191; Cox and Snell R2=0.143).
Table 3
Median split based binary logistic regression analysis of variables significantly associated with the level of knowledge among the Saudi population, a cross-sectional study conducted in Saudi Arabia, June–September 2024 (N=1033)
Sensitivity analysis of alternative knowledge-score thresholds
To evaluate the robustness of the findings based on the median cut-off for defining ‘good knowledge’, sensitivity analyses were conducted using alternative thresholds: the upper 33rd percentile (score ≥18) and the upper 25th percentile (score ≥19). When applying the 33rd percentile, multivariable logistic regression showed results consistent with those of the original model. Sex, working in the healthcare field, smoking status, and the use of ‘other sources’ remained significant predictors of knowledge levels with similar ORs and significance levels (Supplementary file Appendix 3). However, when the 25th percentile threshold was applied, only smoking status and ‘other sources’ remained significant, whereas sex and working in the healthcare field were non-significant (Supplementary file Appendix 4). The explanatory power of this model (Nagelkerke R2=0.119) was lower than that of the original model (R2=0.191). These findings support the median and 33rd percentile thresholds as more stable and meaningful cut-offs for classifying knowledge levels in this population.
DISCUSSION
The findings of the analysis revealed that the main sources of knowledge on the effects of smoking on fracture healing were the internet and healthcare personnel. In addition, binary logistic regression analysis concluded that men had a 52% lower level of knowledge than women, smokers had a 46% lower level of knowledge than non-smokers, and those working in healthcare had a knowledge level almost three times that of those who were not working in healthcare. Furthermore, of the sources of knowledge, those who chose ‘other sources’ showed a significantly higher level of knowledge.
Previous studies have reported higher rates of smoking in men than in women, similar to that reported in this study17,18. Sociocultural norms linking smoking to a masculine image may have been one of the causes of these differences19. In addition, cognitive dissonance, a phenomenon in which individuals avoid information that conflicts with their habits, may have affected smokers’ awareness of the impact of smoking on bone healing20,21. Meanwhile, female participants demonstrated a higher level of understanding of the effects of smoking on general health, which is consistent with the literature assessing general knowledge of the effects of smoking on health and knowledge of other diseases22,23. Despite a Saudi study concluding that men achieved higher levels of perception24, limiting participants between 10 and 34 years of age may explain the differences in our outcomes.
Although the initial univariate analysis suggested that a history of fractures and information obtained from healthcare personnel were significantly associated with the level of knowledge, the multivariable binary logistic regression model revealed that both factors could be confounded by other variables.
Although the internet was considered a main source of knowledge by 84% of our cohort, as well as 62% of participants in a local study conducted in the Eastern Province25, utilizing it as the primary source of information was not significantly related to the observed level of knowledge. This may be attributed to the lower reliability of health information on the internet. A comprehensive meta-narrative systematic review by Daraz et al.26 described online health information as generally suboptimal and unreliable and concluded that the internet is a poor resource in this regard. Similarly, a study by Akerkar et al.27 highlighted that the internet significantly influences healthcare decisions, with over 70% of consumers reporting that online information affects their treatment choices. The quality and reliability of this information remain questionable, with most people failing to critically evaluate online health information, often mistakenly perceiving it as trustworthy and of good quality27.
A study published in the Saudi Medical Journal stated that 51% of the participants trusted health information from social media platforms. According to the study’s findings, 38% of the participants depended on personal experiences provided on these platforms, although these experiences might not be relevant to others28. The implementation of WhatsApp represents the key reason for this particular situation, with governmental reports showing that WhatsApp ranks as the leading social media platform in Saudi Arabia, with 89.9% users29. People cannot verify the reliability of health information that appears on WhatsApp. The study demonstrated that Saudi public users shared health messages on WhatsApp groups through which multiple untrustworthy messages could mislead their audience30.
Although the results highlight the utilization of multiple sources for obtaining smoking-related health information, such as social media, healthcare personnel, and the internet, a large cohort of participants listed ‘other sources’ as the main source of knowledge of smoking-related health risks. A study conducted in 2023 found that 9% of tobacco smokers visited mobile smoking cessation clinics (SCC) and were counseled on the risks associated with smoking, and 60% of tobacco smokers were aware of SCC31. The warning labels displayed on smoking products serve as unspecified sources of knowledge. A European research team found that warning labels directly influence people’s knowledge of smoking risks32. Similarly, the Saudi Arabian government adopted plain tobacco packaging while updating cigarette carton warning labels in January 202033. A double-blind clinical trial demonstrated that mobile applications worked effectively to help people quit smoking34. Future studies should identify and assess the impact of unspecified sources of awareness on smoking and fracture healing.
Strengths and limitations
This study assessed awareness of the effects of smoking on fracture healing in a Saudi Arabian population sample. The strengths of this study include a large sample size, use of a validated assessment tool (SFKAT) with excellent reliability, and robust statistical analysis, including binary logistic regression, to adjust for confounders. However, the potential selection bias due to social media recruitment may have overrepresented younger and more educated individuals, which may have overestimated the results. Furthermore, this method may have excluded older populations, rural citizens, and other less digitally connected individuals. Relying on self-reported data may have introduced response bias. In addition, the cross-sectional design only accounts for associations and does not provide causal relationships between the exposure and outcome variables. Although binary logistic regression was implemented to adjust for confounders, residual or unmeasured confounding effects remained unadjusted. The study was conducted in a Saudi Arabian population; hence, the generalizability of the results to other populations may be limited. In addition, the moderate construct validity of some items within the SFKAT was another key limiting factor in this study, as five of the ten items had factor loadings below 0.4, which suggests that these questions may not have a strong alignment with the underlying knowledge construct. This may have lowered the overall precision of the SFKAT in measuring public awareness, potentially diluting the observed associations or misclassifying knowledge levels. To detect subgroup-specific differences in associations, the potential interaction effects (such as between sex and smoking status or sex and working in the healthcare field) need to be analyzed, which were not included in the final regression model. Our primary objective was to identify independent predictors of knowledge. Due to a lack of previous literature and hypotheses, the analysis was performed preliminarily on these factors without testing further subgroups within such factors. Additionally, although the median SFKAT score was used as the main threshold to classify participants into knowledge groups, we conducted a sensitivity analysis using alternative cut-off points (upper 33rd and 25th percentiles) to evaluate the robustness of our classification. The 33rd percentile model yielded results consistent with those of the main model, preserving the significance and direction of the key predictors. However, using the upper 25th percentile as a stricter cut-off altered the statistical significance of some predictors and reduced the model’s explanatory power. These findings support the validity of using the median-based classification while acknowledging that stricter definitions of ‘good knowledge’ may produce less stable models. Future research should address these limitations through more tool refinement and robust population sampling.
CONCLUSIONS
The knowledge regarding the damaging effects of smoking on fracture healing is suboptimal, especially among men and smokers. Further, sex, healthcare work, and smoking status were determinants of knowledge level. Effective educational programs combined with counseling strategies should be developed to address existing knowledge deficits.