INTRODUCTION
Smoking-attributed mortality is increasing steadily in most developing countries1-3. In China, with 20% of the world’s population consuming 40% of the world’s cigarettes, smoking-attributed deaths will continue to increase over the next decades. Prospective studies from developed countries and districts provide strong quantitative evidence that quitting smoking results in better health outcomes4-8. The Hong Kong Lifestyle and Mortality (HK LIMOR) Study, China, found that longer durations of smoking cessation were associated with progressively lower mortality rates from the diseases of interest, and younger age of quitting (25–44 or 45–64 years) appeared to be associated with greater protection: RR was 0.58 (0.38–0.88) and 0.71 (0.54–0.93)8. The earlier women quit smoking, the lower the risk of death from lung cancer or other tobacco-related diseases4. There is limited evidence from low- and middle-income countries (LMICs) about the effects of smoking cessation9. In populations where the risks among smokers are still rising, comparison of current mortality rates among smokers and ex-smokers would underestimate the benefits of quitting.
Tianjin is the third largest city (about 15.6 million inhabitants) after Beijing and Shanghai in China. The death registration system in Tianjin is the first and only death registration system which is collecting the smoking information of the deceased in China. Starting at the end of 2009, the current research group has been collecting information routinely on smokers including: smoking status (current smoking, quit smoking, never smoked); cigarettes/day; and years of smoking recorded on the death certificate10,11. In 2015, in order to further improve the collection of data, smoking information about the duration of smoking cessation was added (if the deceased had quit, the duration of smoking abstinence in years).
The mortality case-control study design, which assesses retrospectively a large number of people who have died by assessing their previous smoking habits from interviewing the family and by recording the underlying disease that caused death, can be used to assess and monitor rapidly and periodically the mortality risks of smoking, and measure the effects of tobacco control actions for a regional or national region. This study evaluated the effect of quitting smoking on mortality in Tianjin city, China.
METHODS
We included all the deaths from ages 35 to 79 years during 2016–2017. The data collection and quality have been described elsewhere10-12. Briefly, the local regulation requires death certification to be completed and entered into the surveillance system by doctors of all hospitals and community health service centers in Tianjin. The public health doctors in district or county CDCs oversee and check the daily reported deaths. Deaths outside hospitals are included in the CDRS based on the information obtained from household interviews and home visits by community clinicians using verbal autopsy as recommended by the World Health Organization. The district or county CDCs are responsible for collecting and verifying the medical certificates for all deaths not occurring in hospitals and adding those deaths to the CDRS weekly, and coding the cause of death according to the ICD-10. The district or county CDCs and TJCDC both carry out data verification, investigation of missing reports, quality control and checking the completeness of the information on the cause and the underlying cause of death codes and data analysis. The proportion of inaccurate coding was <3.5% from 2010 through 2014. On average, 4.5% of the death certificates had missing data about smoking, and this was only 1.6% in 2014.
We excluded deaths among those ≤34 years because smoking was expected to cause very few deaths at a young age, and deaths at ≥80 years as causes of death are less reliable. We followed the methods of Sitas et al.13, using the same diseases to define cases and controls. Cases were deaths from diseases that are causally or strongly associated with smoking, such as cancer of the lung; other cancers related to smoking, such as cancer of mouth, pharynx, larynx, esophagus, or stomach; cardiovascular diseases; COPD; and other. Controls were deaths from all other specified diseases that were not confirmed to be caused by or were not strongly associated with smoking. Excluded were smokers who died from homicide or via an accident or any other unrelated reason, and ill-defined or unknown causes. Underlying causes of death and ICD-10 codes for the cases and controls were according to Sitas et al.13 (Supplementary file Table 1 shows the detail description of each group). This study was implemented as a register-based study based on anonymous data at a local department and was approved by the local department Ethics Committee. Register-based studies on anonymous data do not require written consent in Tianjin.
Table 1
Duration of smoking cessation and mortality from four smoking-related diseases, mortality rate ratios (RRs) comparing ex-smokers or never smokers versus current smokers, and deaths from selected diseases versus deaths from control diseases (both sexes), 2016–2017, Tianjin, China
| Current smokers | Duration of quitting | Trend p* | Never smokers | |||
|---|---|---|---|---|---|---|
| Age (years) | RR (n) | 1–5 years RR (n) 95% CI | 6–9 years RR (n) 95% CI | ≥10 years RR (n) 95% CI | RR (n) | |
| Lung cancer | ||||||
| 35–59 | 1.00 (868) | 1.15 (226) | 0.27 (8) | 0.44 (28) | 0.000 | 0.35 (840) |
| 0.93–1.43 | 0.12–0.59 | 0.28–0.71 | 0.31–0.39 | |||
| 60–69 | 1.00 (1687) | 0.90 (444) | 0.61 (56) | 0.43 (148) | 0.000 | 0.26 (1457) |
| 0.76–1.07 | 0.41–0.90 | 0.34–0.54 | 0.24–0.29 | |||
| 70–79 | 1.00 (1853) | 0.86 (471) | 0.75 (84) | 0.50 (374) | 0.000 | 0.24 (1712) |
| 0.72–1.01 | 0.53–1.06 | 0.42–0.58 | 0.22–0.27 | |||
| Other smoking-related cancers | ||||||
| 35–59 | 1.00 (1001) | 0.76 (172) | 0.47 (16) | 0.56 (41) | 0.183 | 0.44 (1263) |
| 0.61–0.95 | 0.25–0.87 | 0.37–0.84 | 0.39–0.49 | |||
| 60–69 | 1.00 (1097) | 0.81 (265) | 0.51 (80) | 0.54 (116) | 0.003 | 0. 46 (1035) |
| 0.67–0.99 | 0.32–0.81 | 0.42–0.69 | 0.41–0.51 | |||
| 70–79 | 1.00 (736) | 0.73 (162) | 0.44 (20) | 0.69 (211) | 0.787 | 0.63 (1796) |
| 0.59–0.91 | 0.26–0.74 | 0.57–0.84 | 0.56–0.70 | |||
| Cardiovascular disease | ||||||
| 35–59 | 1.00 (3269) | 0.46 (322) | 0.72 (74) | 0.63 (130) | 0.070 | 0.40 (3846) |
| 0.38–0.56 | 0.47–1.12 | 0.46–0.87 | 0.37–0.44 | |||
| 60–69 | 1.00 (3413) | 0.65 (616) | 0.98 (175) | 0.83 (538) | 0.016 | 0.62 (7041) |
| 0.55–0.76 | 0.71–1.36 | 0.69–1.00 | 0.57–0.68 | |||
| 70–79 | 1.00 (4111) | 0.78 (946) | 0.94 (233) | 0.87 (1422) | 0.295 | 0.85 (13356) |
| 0.67–0.91 | 0.70–1.28 | 0.76–0.99 | 0.78–0.92 | |||
| COPD | ||||||
| 35–59 | 1.00 (81) | 0.72 (13) | 0 | 1.84 (11) | 0.028 | 0.81 (177) |
| 0.39–1.33 | - | 0.92–3.68 | 0.61–1.06 | |||
| 60–69 | 1.00 (184) | 1.02 (52) | 1.16 (11) | 1.45 (53) | 0.056 | 0.62 (368) |
| 0.73–1.44 | 0.59–2.29 | 1.02–2.05 | 0.51–0.76 | |||
| 70–79 | 1.00 (473) | 0.83 (115) | 1.29 (38) | 1.07 (206) | 0.065 | 0.55 (972) |
| 0.64–1.06 | 0.84–1.99 | 0.87–1.32 | 0.48–0.63 | |||
| All deaths of interest | ||||||
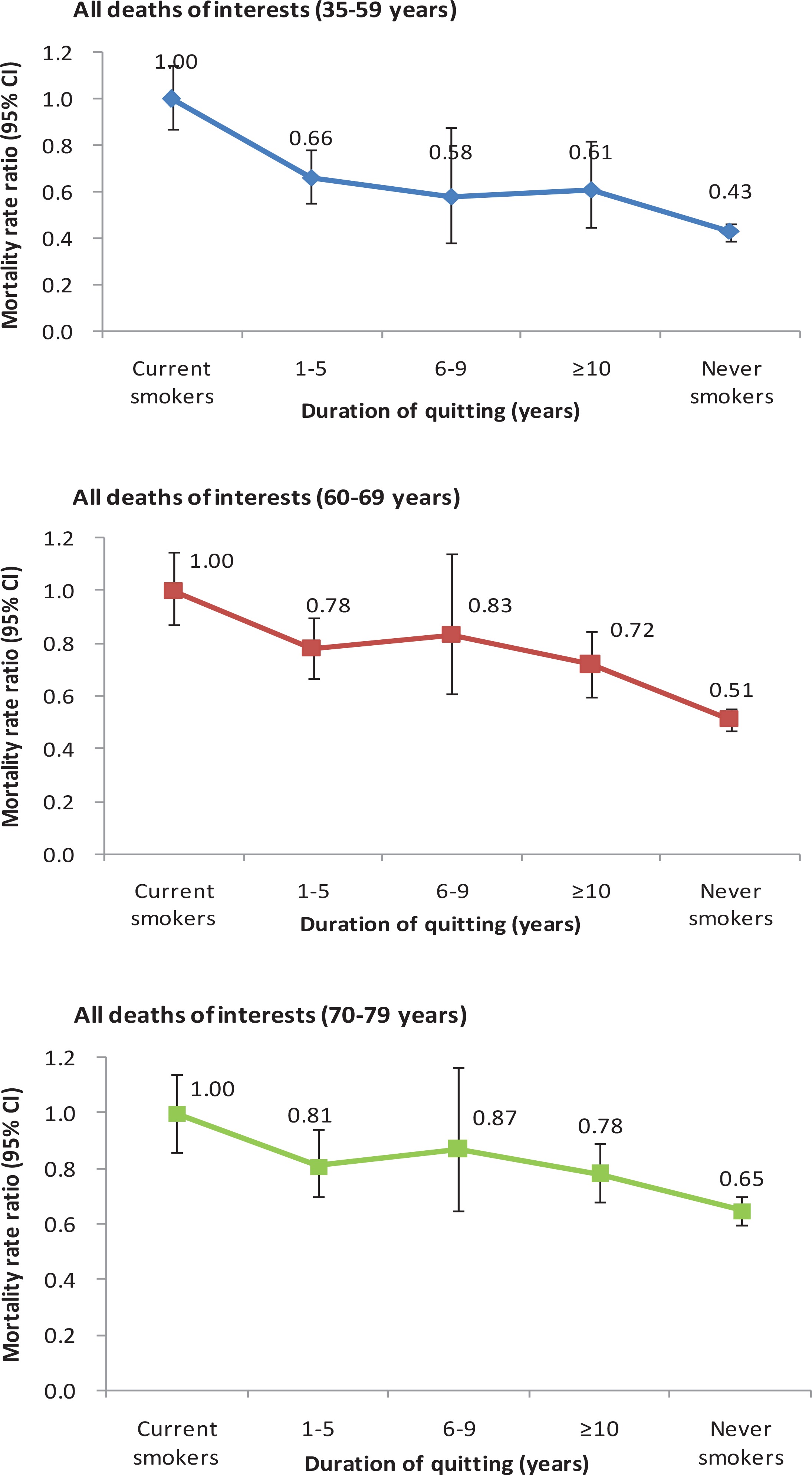
| 35–59 | 1.00 (5393) | 0.66 (779) | 0.58 (102) | 0.61 (223) | 0.000 | 0.43 (6631) |
| 0.55–0.78 | 0.38–0.88 | 0.45–0.82 | 0.39–0.46 | |||
| 60–69 | 1.00 (6644) | 0.78 (1454) | 0.83 (295) | 0.72 (914) | 0.000 | 0.51 (11139) |
| 0.67–0.90 | 0.61–1.14 | 0.60–0.85 | 0.47–0.55 | |||
| 70–79 | 1.00 (7496) | 0.81 (1802) | 0.87 (395) | 0.78 (2354) | 0.001 | 0.65 (18790) |
| 0.70–0.94 | 0.65–1.17 | 0.68–0.89 | 0.60–0.70 | |||
Statistical analysis
Case versus control odds ratios for the quitting status were calculated by unmatched multiple logistic regression, adjusted for 5-year age groups, sex and education (none, primary, higher, do not know), marital status (never, widowed, divorced, married or living as married, do not know) and are described as mortality rate ratios (RRs, calculated as odds ratios). Statistical tests and 2-sided 95% confidence intervals (CIs) were based on changes in log-likelihood. When the 95% CI for the relative risk in men did not overlap with that in women, the sex difference was significant at p<0.05 level.
To assess the association of smoking cessation with smoking-attributed mortality by age of quitting, the RR was calculated for never smokers, and quitters who stopped smoking at the ages of 25–44 and 45–64 years8, compared with current smokers. To select the appropriate age range, mortality RRs were calculated for main cause-specific deaths by smoking history (ever vs never smokers) in all deaths. All analyses were conducted in 2019 using SPSS 23.0.
RESULTS
Mortality by the duration since quitting
There were 41072 male and 24226 female cases, and 6723 male and 6804 female controls. The demographic characteristics of the underlying causes of death among cases and controls in different age groups in Tianjin from 2016 to 2017 were similar, with a mean (SD) age of 67.17 (9.35) and 64.88 (10.08) years, respectively (Supplementary file Table 2).
Table 1 shows that in the 35–59 years age group, RRs among long-term quitters (vs current smokers) were lower: RR was 0.44 (95% CI: 0.28–0.71) for lung cancer, 0.56 (95% CI: 0.37–0.84) for smoking-related cancer, 0.63 (95% CI: 0.46–0.87) for cardiovascular disease (CVD), and 1.84 (95% CI: 0.92–3.68) for COPD. Quitters who had stopped for 6–9 years also had lower lung cancer, smoking-related cancer mortality risks compared with current smokers, but the same mortality risk in CVD and COPD. New quitters who had stopped for <6 years had lower other smoking-related cancer and CVD mortality risks: RR was 0.46 (95% CI: 0.38–0.56) in the 35–59 years age group, 0.65 (95% CI: 0.55–0.76) for 60–69 years and 0.78 (95% CI: 0.67–0.91) for 70–79 years, for CVD; RR was 0.76 (95% CI: 0.61–0.95) in the 35–59 years age group, 0.81 (95% CI: 0.67–0.99) for 60–69 years and 0.73 (95% CI: 0.59–0.91) for 70–79 years, for other smoking-related cancers. However, the RRs for lung cancer and COPD among new quitters were similar to those of current smokers in all the age groups.
Figure 1 shows declining trends of RRs for all deaths of interest from current smoking to quitting for <1–5, 6–9 and ≥10 years, and never smoking in all three age groups.
Mortality by age of quitting
Table 2 shows mortality RRs for the other four disease groupings (causable by smoking) by age of quitting versus current smoking. Few quitters stopped before the age of 45 years, so the estimates of quitting at the age of 25–44 years in old age are not statistically reliable. Among subjects who had stopped at age 45–64 years, the RRs for lung cancer, smoking-related cancers and CVD were lower, but those for COPD were similar to current smokers.
Table 2
Age at smoking cessation and mortality from four smoking-related diseases, mortality rate ratios (RRs) comparing ex-smokers or never smokers versus current smokers, 2016–2017, Tianjin, China
| Current smokers | Age at quitting (years) | Trend p* | Never smokers | |||
|---|---|---|---|---|---|---|
| Age (years) | RR (n) | 25–44 RR (n) 95% CI | 45–64 RR (n) 95% CI | RR (n) | ||
| Lung cancer | ||||||
| 35–59 | 1.00 (868) | 0.73 (36) | 0.98 (225) | <0.001 | 0.35 (840) | |
| 0.82–1.21 | 0.47–1.13 | 0.77–1.18 | 0.31–0.39 | |||
| 60–69 | 1.00 (1687) | 0.51 (22) | 0.64 (480) | 0 | 0.26 (1457) | |
| 0.83–1.21 | 0.28–0.93 | 0.55–0.75 | 0.24–0.29 | |||
| 70–79 | 1.00 (1853) | 0.35 (23) | 0.54 (290) | 0.003 | 0.24 (1712) | |
| 0.21–0.60 | 0.45–0.55 | 0.22–0.27 | ||||
| Other smoking-related cancers | ||||||
| 35–59 | 1.00 (1001) | 0.57 (37) | 0.73 (192) | 0.036 | 0.44 (1263) | |
| 0.83–1.20 | 0.37–0.87 | 0.58–0.90 | 0.39–0.49 | |||
| 60–69 | 1.00 (1097) | 1.33 (27) | 0.61 (312) | 0.588 | 0. 46 (1035) | |
| 0.81–1.23 | 0.78–2.27 | 0.52–0.73 | 0.41–0.51 | |||
| 70–79 | 1.00 (736) | 0.25 (7) | 0.69 (154) | 0.147 | 0.63 (1796) | |
| 0.11–0.57 | 0.55–0.86 | 0.56–0.70 | ||||
| Cardiovascular disease | ||||||
| 35–59 | 1.00 (3269) | 0.47 (121) | 0.54 (401) | 0.862 | 0.40 (3846) | |
| 0.82–1.22 | 0.35–0.65 | 0.45–0.65 | 0.37–0.44 | |||
| 60–69 | 1.00 (3413) | 1.00 (82) | 0.75 (1101) | 0.115 | 0.62 (7041) | |
| 0.83–1.20 | 0.63–1.60 | 0.65–0.86 | 0.57–0.68 | |||
| 70–79 | 1.00 (4111) | 0.64 (88) | 0.87 (1008) | 0.305 | 0.85 (13356) | |
| 0.42–0.96 | 0.75–1.02 | 0.78–0.92 | ||||
| COPD | ||||||
| 35–59 | 1.00 (81) | 2.42 (10) | 0.58 (13) | 0.047 | 0.81 (177) | |
| 0.75–1.34 | 1.14–5.13 | 0.32–1.08 | 0.61–1.06 | |||
| 60–69 | 1.00 (184) | 1.33 (6) | 1.23 (98) | 0.392 | 0.62 (368) | |
| 0.79–1.27 | 0.53–3.35 | 0.94–1.62 | 0.51–0.76 | |||
| 70–79 | 1.00 (473) | 0.66 (10) | 1.15 (151) | 0.966 | 0.55 (972) | |
| 0.32–1.37 | 0.91–1.45 | 0.48–0.63 | ||||
| All deaths of interest | ||||||
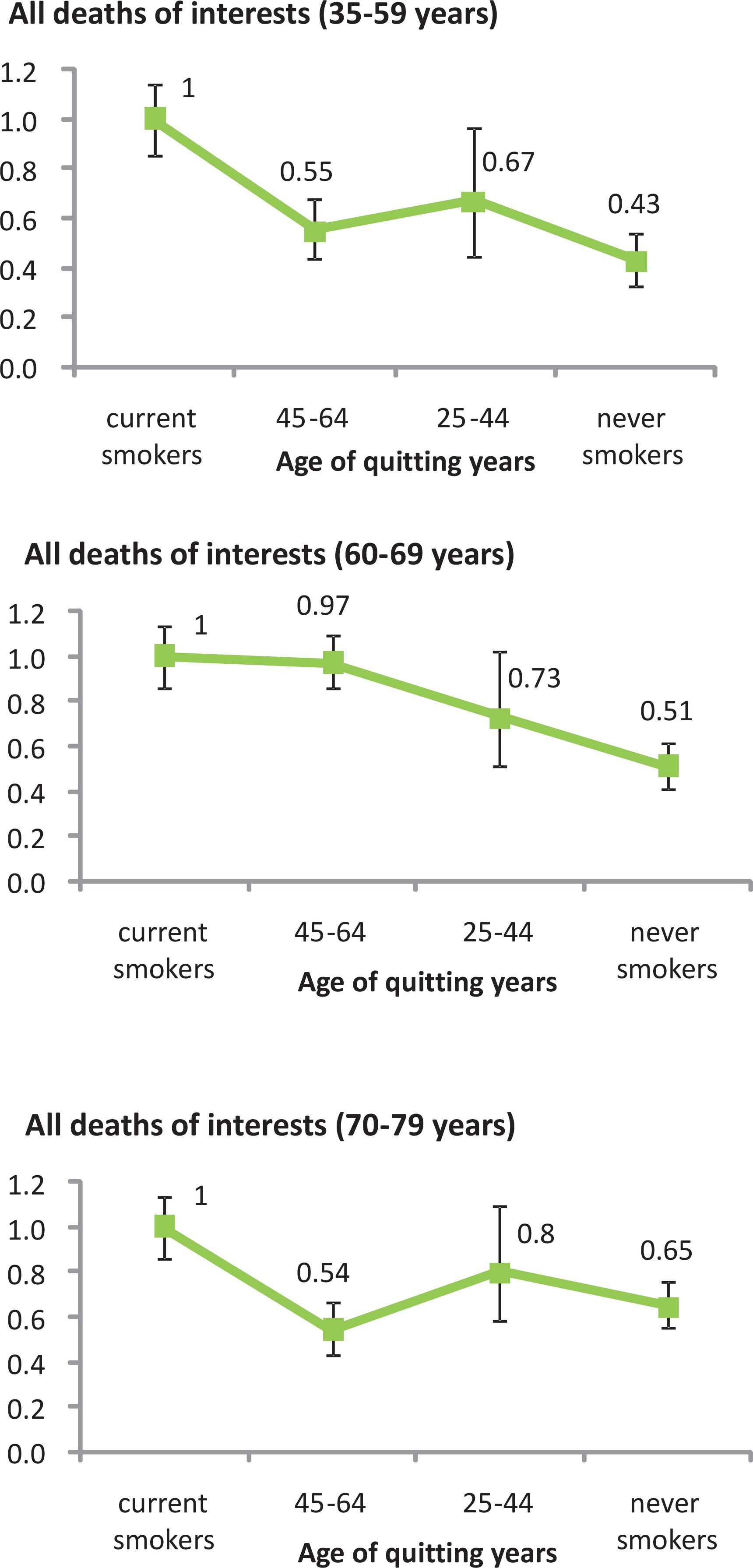
| 35–59 | 1.00 (5393) | 0.55 (221) | 0.67 (877) | 0.000 | 0.43 (6631) | |
| 0.75–1.34 | 0.42–0.74 | 0.56–0.79 | 0.39–0.46 | |||
| 60–69 | 1.00 (6644) | 0.97 (158) | 0.73 (2123) | 0.000 | 0.51 (11139) | |
| 0.79–1.27 | 0.63–1.52 | 0.65–0.83 | 0.47–0.55 | |||
| 70–79 | 1.00 (7496) | 0.54 (141) | 0.80 (1712) | 0.000 | 0.65 (18790) | |
| 0.37–0.80 | 0.69–0.93 | 0.60–0.70 | ||||
Figure 2 also shows a clear declining trend of mortality risk, from current smoking to quitting at the ages of 45–64 and 25–44 years and never smoking, for all deaths of interest at age 35–59 years: RR was 1.00 (95% CI: 0.75–1.34), 0.55 (95% CI: 0.42–0.74), 0.67 (95% CI: 0.56–0.79) and 0.43 (95% CI: 0.39–0.46) (linear trend p=0.000). The same trend was found at age 60–69 years. However, subjects at age 60–69 years who stopped at younger age (25–44 years) had same mortality risks with current smokers: 0.97 (95% CI: 0.63–1.52).
DISCUSSION
Our research clearly demonstrates the protective effect of smoking cessation on mortality. No similar studies have been retrieved for mainland China. The benefits of quitting and of longer durations of smoking cessation, associated with progressively lower mortality rates of the diseases of interest, can be observed by using the mortality case-control study design.
Patients who died of lung cancer, and with a duration of quitting of 1–5 years, had a risk of death similar to that of smokers. The strong protective effect against mortality can only be observed when the duration of quitting is >10 years. This may be related to the fact that the vast majority of the patients who have given up smoking for a short period of time did so because of illness. Therefore, in future surveillance, the non-communicable diseases incidence surveillance system can be linked to the all-cause of death surveillance system, and the main reason for quitting smoking can be judged by the disease onset time. Unlike lung cancer, the effect of smoking cessation on the risk of cardiovascular death is evident in a relatively short period of time. In all age groups in this study, the risk of cardiovascular death is significantly reduced in people who quit smoking for 1–5 years.
The patients who died of COPD were also a group whose smoking cessation effect was not obvious, which was consistent with the results of many cohort studies. COPD usually occurs among smokers, whose respiratory symptoms have worsened over the years, during which most people may need to quit smoking because of their worsening condition14. Therefore, for COPD, the reverse causal effect of smoking cessation is more common, especially in older people with longer smoking time and symptoms and lower recovery ability. In the current analysis, there is a reverse causal relationship among the 60–69 years age group who have quit smoking for >10 years and died of COPD.
Tianjin is the third largest city of China, and also the national central city and mega-city, the economic center of Bohai Rim Area with an area of 11920 km2. The first cigarette factory in China was established in Tianjin in 1891 by Beiyang Tobacco Company and the industry there controlled more than 70% of the country’s cigarette market15. Tianjin people were among the first to smoke in large numbers in China.
The first China National Smoking Prevalence in 1984 showed that the smoking prevalence in Tianjin was 61.99% in men and 7.04% in women16. The latter was the highest in China. The tobacco epidemic was still high in Tianjin17. Stopping smoking is one of the most practical ways to avoid a large proportion of smoking-attributable deaths, particularly premature deaths (age 35–69 years).
Quitting is not common on the Chinese mainland. Ex-smokers are far fewer than current smokers, particularly those who stopped smoking at a young age (≤45 years). However, with increasing smoking cessation from more effective tobacco-control measures in developing regions, the applicability of the mortality case-control studies should expand. Moreover, many high-income countries also have no or limited prospective data showing the harms of smoking and the benefits of quitting at a country level. Mortality case-control studies can provide evidence that smoking kills, and our present study has shown that this study design could also provide evidence that smoking cessation is effective in populations with reasonably reliable underlying causes of deaths, by collecting data about smoking and the duration of quitting up to the time of death. Evidence of the health benefits of quitting is needed to support strong tobacco control policies and provide smoking cessation services, and to motivate people to quit before illnesses occur. The health benefits of quitting can be observed by using the mortality case control study design. In countries, regions or cities with a reliable system of death certification, the mortality case-control study design using routinely collected smoking data from death certificates can be used to assess and monitor periodically the mortality risks and quit-benefit of smoking, and evaluate the effects of tobacco control measures at different stages of the tobacco epidemic.
Limitations
Several limitations of our study should be considered. First, the definitions of cases and controls in previous proportional mortality studies varies. For example, some diseases such as breast cancer and colorectal cancer are considered to be causally related to smoking according to the 2014 USSG Report18, but were defined as controls in our study. Smoking was associated with reduced risk of Parkinson’s disease, ulcerative colitis and endometrial cancer19, but we analyzed them as cases. Nonetheless, there is no consensus of the definitions of cases and controls in mortality case-control studies. Further research is warranted to determine the most appropriate definition for studying smoking or other factors within this study design. There was a fairly large disproportion in numbers between the cases and the controls in our study, because our study was in a natural population, we should not choose the matching method to select a 1:1 control for the case, or delete some cases for the control, which will lose a lot of valuable information and cause bias. But the disproportion did not affect the accuracy of the analysis. Our control group smoking prevalence was a little lower than those in the Behavioral Risk Factor Surveillance System (BRFSS) in the Tianjin population (TJCDC, unpublished data, 2010–2012, a representative study of the whole population in Tianjin). In our study, any biases of exposure data for controls (including recall bias) should have similarly affected the cases.
CONCLUSIONS
The mortality case-control study design using routinely collected smoking data from death certificates can be a quick, efficient and reliable method to assess and monitor mortality risks of smoking in other cities or countries with a reliable system of death certification and good quality control measures as in Tianjin. Tianjin has been collecting information routinely on smoking of the deceased on the death certificate from 2010. We found that the longer durations of smoking cessation are associated with progressively lower mortality rates from the diseases of interest. Among the patients who died of lung cancer, the strong protective effect can only be observed when the duration of quitting is ≥10 years. The effect of smoking cessation on the risk of death from cardiovascular disease can be observed when the duration of quitting is 1–5 years.