

INTRODUCTION
Pandemic-related disruptions to daily routines have impacted multiple behavioral measures and health conditions, particularly during the peak of the lockdown period1. Tobacco users are at higher risk of more severe COVID-19 outcomes2. As a result, the COVID-19 pandemic should be considered an urgent priority in tobacco control efforts to reduce tobacco consumption, make tobacco users aware of their high risks, and create campaigns to target tobacco cessation. However, it should be noted that other stressors resulting from the pandemic and related lockdown orders, such as increased anxiety, social isolation, and economic concerns, may have increased. As a result, these stressors may lead to an increase in the initiation of tobacco use by non-users and/or increased product use among current users3. As a result, it is essential to understand how pandemic-related lockdown measures have impacted tobacco-related behavior.
According to data from the World Health Organization (WHO), smoking causes the deaths of 8 million people per year, where 7 million deaths are caused by the direct use of tobacco, and the rest from passive smoking4. Moreover, there is the misconception that waterpipes are less harmful than cigarettes5. Waterpipe smokers are more likely to be exposed to CO (carbon monoxide) than cigarette smokers. Yet, cigarettes and waterpipes have the same end products that contain cancer-causing chemicals (carcinogens) and nicotine that leads to addiction6. One waterpipe session is equivalent to smoking 100 cigarettes7.
Besides, people who are passive smokers breathe in the smoke from burning cigarettes that smokers exhale. Most exposure to passive smoking occurs in homes, cars, and public spaces8. Therefore, passive smoking increases the risk of tobacco-related diseases among adults and children. One systemic review conducted among university students from several Arab countries found that smoking rates (cigarettes and waterpipe) were highest in Egypt, Kuwait, and Kingdom of Saudi Arabia, with higher smoking prevalence among males than females in Yemen, Bahrain, Tunisia, Egypt, Palestine, Syria, and Jordan, with significant differences between the countries9. Another study on smoking among young people in 16 Arab countries indicated that 10.6% of the participants were current waterpipe smokers, with the highest rate being in Lebanon (34.2%) and the lowest in Oman (9%). Overall, the study indicated that boys were more likely than girls to smoke waterpipes in Palestine, Lebanon, and Jordan (43.8%, 38.6%, and 25.7%, respectively)10.
Tobacco smokers are at high risk of severe COVID-192 due to chronic lung diseases, weak immunity, cross-infection as the smokers might share devices between them as most of the waterpipes are smoked socially with others, and poor hygiene practices11. Waterpipe is often used with a shared mouthpiece smoking instrument between smokers, which increases the risk of viral transmission12. One systematic review study found that smokers were 1.4 times more likely (RR=1.4; 95% CI: 0.98–2.00) to have severe symptoms of COVID-19, in addition, close to 2.4 times more likely to be admitted to an ICU, might need mechanical ventilation or even die compared to non-smokers (RR=2.4; 95% CI: 1.43–4.04)13.
Several contributing factors among smokers that can increase the severity of COVID-19 include age, gender, level of education, nationality, and body health status14. It is suggested that certain factors such as income, employment, medical conditions, location, and access to healthcare have links to different races, ethnicity, and nationalities, and thus influence the COVID-19 severity15. One descriptive study has quantified the impacts of quarantine on behaviors related to weight gain and obesity. The average BMI of the participants was 27 kg/m2, and almost all of the participants reported staying home more often than before the pandemic. Gaining weight of 5–6 kg was reported by 22% of the sample16. Moreover, another cross-sectional study conducted during the COVID-19 quarantine involved 407 Lebanese participants in order to measure the behavioral features of eating and found that the BMI was higher during quarantine17. Another study conducted during the lockdown in the United Arab Emirates (UAE) concerning food intake and decreased physical activity, found that an increase in weight often lead to an increase in smoking frequency. Thus, all these factors may increase the vulnerability of COVID-19 and worsen the severity of the disease18.
In relation to the pandemic and smoking practices, a study conducted in Ohio during the early pandemic period measured the perceived risk of infection associated with indoor smoking and found that the desire to quit among smokers during the outbreak was related to the perceived risk of COVI-19 infection and diabetes19. While on the other hand, another national study conducted in the UK revealed that the psychosocial stress of the pandemic increased the prevalence of smoking and had more effect on former smokers20. In addition, a meta-study conducted in 2020 found a significant association between smoking and the progression of COVID-19 infection21.
Studying the impact of lockdown on various populations and age groups revealed that the lockdown had a negative effect on elderly peoples’ feelings of loneliness, isolation, and despair22. Therefore, our study aims to assess the impact of the COVID-19 lockdown on smoking practices (cigarettes and waterpipe) and to identify the associations with selected sociodemographic factors, working status, and BMI. As far as we know, there has not been a thorough study on the relationship between lockdown and smoking behaviors and BMI in Arab countries.
METHODS
Study design and settings
A retrospective observational study with a cross-sectional design using an online validated survey was launched originally in 38 different countries, and information collected from 37207 participants. The Eastern Mediterranean Region (WHO-EMR countries) data related to 10 Arab countries (United Arab Emirates, Lebanon, Bahrain, Egypt, Jordan, Kuwait, Oman, Qatar, Saudi Arabia, and Palestine) were selected for analysis in this study. The international study protocol was approved by the Ethics Committee for the Social Sciences and Humanities of the University of Antwerp (Ref no: SHW_20_46). The survey was kept open between 17 April and 25 June 2020. The details of the study methodology have been described elsewhere23-25. In addition to the international ethical approval and the approval from the Ethics Advisory Committee on Social and Human Sciences of the University of Antwerp, ethical approval was sought on 26 April 2020 from Zayed university Ethics Committee before data collection (Ref. No.: ZU20_098_F). Before moving on to the survey question, respondents had to read the following: 1) what the study is about (objective); 2) who can participate; 3) what are the rights and responsibilities; and 4) the contact details of the principal investigators. Finally, they were asked to provide informed consent and say whether they were aged ≥18 years, immediately after the survey’s welcome page (https://osf.io/r9n25/, accessed on 15 July 2022).
Population and sampling
Participants included in this study were aged ≥18 years, of both genders, and residing in any participating Arab country; those aged <18 years were excluded from this study. Convenience snowball sampling was used to recruit participants, and advertisements for the survey were conducted using different social network platforms, in addition to the research team’s academic networks, university mailings, and stakeholders. First, the international research team created and shared multiple social media banners on sites such as Facebook, Twitter, Instagram, Snapchat, and LinkedIn in both private and public online groups. Furthermore, an international press release was distributed to the spokespersons of the research teams in each country, who were able to distribute it to their local press. In addition, the international news agency Reuters produced a video article about the Corona Cooking Survey, which was distributed to several international press organizations. The Corona Cooking Survey was mentioned in newspapers, on radio or on news websites in 24 different countries, so it was helpful to share the link to a global web page where participants could find the right survey link for their own country23-25.
Measurements, instruments, and tools of data collection
The questionnaire was a self-administered, validated, and the online survey was conducted using the software Qualtrics and took approximately 20 minutes to complete. All countries used the same survey structure as a starting point. Extra questions were added at the end of the questionnaire, and some questions were adapted to better reflect the sociocultural background (e.g. alcohol use in Arab countries). An ad hoc questionnaire, created for the present study, took into account items from other questionnaires such as Health Behavior in School-aged Children (HBSC) (http://www.hbsc.org/methods/, accessed on 15 July 2022). Moreover, to ensure the questionnaire was valid and reliable, the survey questionnaire and the additional questions were reviewed and discussed by all principal researchers of the 10 Arab countries that participated in this study via several ZOOM meetings and WhatsApp groups created for this research project.
The complete questionnaire consisted of six main parts in addition to the additional questions specific to each country or region: 1) profiling questions; 2) lockdown and consequences; 3) general food behavior; 4) grocery shopping; 5) cooking and baking; and 6) eating behavior. The last part of the questionnaire used in the 10 Arab countries included additional questions about dieting, physical (in)activity, body image, smoking behaviors (cigarettes and waterpipes), and self-reported weight and height. The reported body mass index (BMI, kg/m2) was categorized according to the WHO criteria into: underweight (<18.5), normal (18.5–24.9), overweight (25–29.9) and obese (≥30)26.
The survey questions were available in native Arabic and English, extending choices for the respondents. A total of 12433 participants, from 10 Arab countries, who reported their smoking behavior before and during COVID-19 confinement were included in this analysis. Changes in smoking behaviors during the COVID-19 confinement were analyzed and compared according to selected sociodemographic factors (gender, age, education level, and working status) and BMI.
Statistical analysis
A χ2 test was used to compare categorical variables/groups before and during the lockdown. A binary logistic regression analysis was conducted to assess the association between smoking before and during the COVID-19 pandemic and the associated independent variables, including age groups, physical activity, country, educational level, gender, work status, and watching TV. Odds ratios (ORs) and their 95% confidence intervals (CIs) were used as indicators of levels of association. A p<0.05 was considered statistically significant. Statistical analysis was conducted on IBM SPSS Statistics, Version 25 (IBM, Armonk, NY, USA)27.
RESULTS
Prevalence of smoking by country
Table 1, which compares smoking prevalence across the 10 Arab countries included in this study, shows that the overall smoking prevalence rate was 30% prior to lockdown and decreased to 24% during the lockdown. Before the lockdown, the highest prevalence was in Jordan, Lebanon, and Palestine (38%, 38%, and 33%, respectively), and the lowest was in Oman (10%). While during the lockdown, the highest prevalence of smoking was in Lebanon (33%), and the lowest was in Oman (8%). Before the lockdown, the prevalence rate of cigarettes smoked daily (more than once) was 28%, with Egypt having the highest rate (42%) and Jordan and Palestine having the lowest (26% and 26%, respectively). However, during the lockdown, there was an increase in the prevalence rate of cigarettes smoked daily (more than once) to 32%, with Egypt having the highest rate (56%). Before the lockdown, the prevalence of waterpipe smoking (more than once a week and more than once a day) was 46.4% across all countries. It increased during the lockdown to 54%, with Lebanon, Jordan, and Palestine having the highest prevalence. There was a statistically significant difference between the countries (Lebanon, Palestine, and Jordan) and smoking (p<0.001), (Table 1).
Table 1
Smoking practices (cigarettes and waterpipes) before and during COVID-19 lockdown among participants of 10 Arab countries, 2020 (N=12433)
Prevalence of smoking by gender
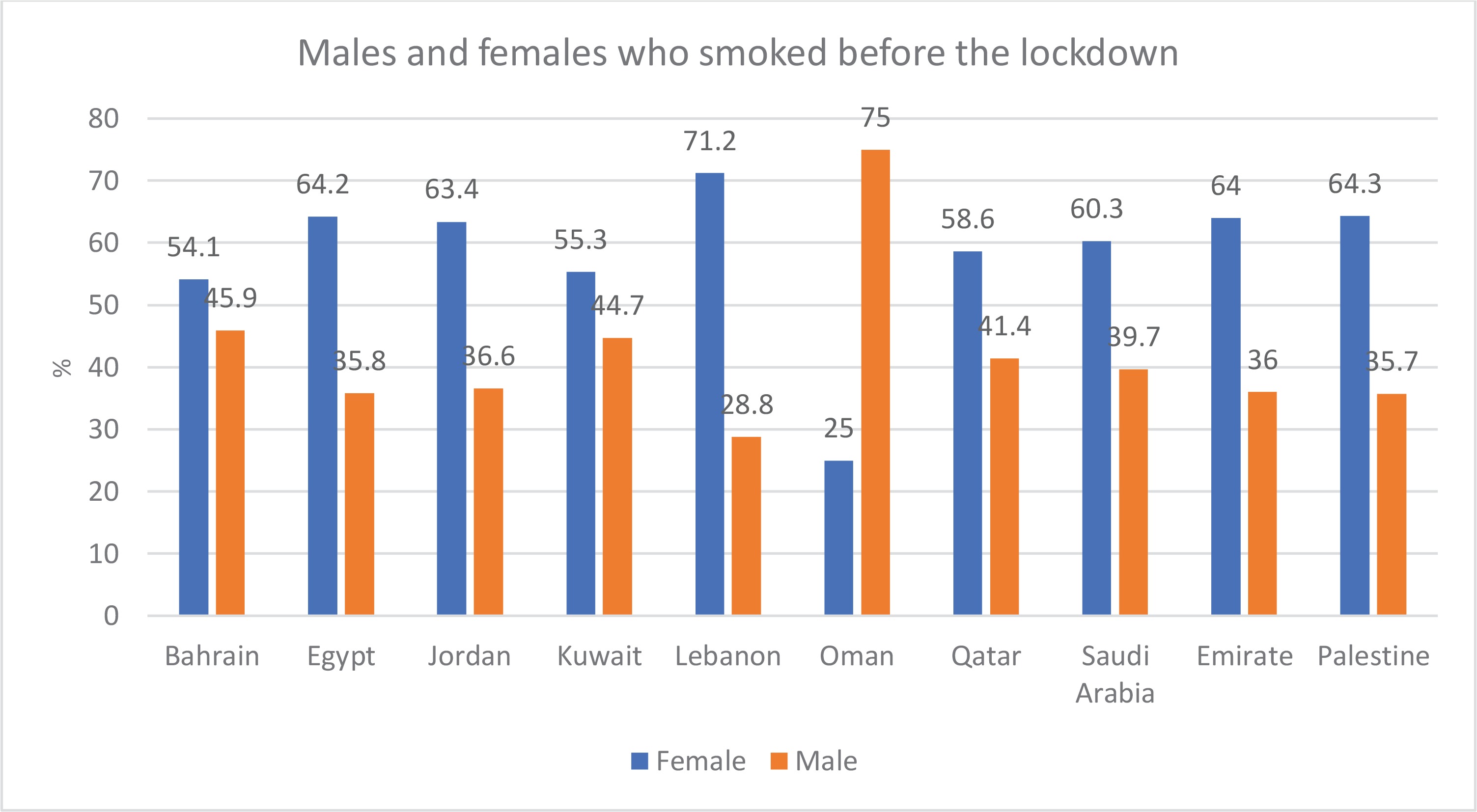
According to the data, the prevalence of female smokers was highest in Lebanon (71%), followed by Palestine (64%), Egypt (64%), the United Arab Emirates (64%), Jordan (63%), Saudi Arabia (60%), Qatar (58.6%), Kuwait (55%), and Bahrain (54%), and the lowest was in Oman (25%). On the other hand, the percentage of males who smoked before the lockdown was higher in Oman (75%) only (Figure 1).
During the lockdown, Lebanon had the highest percentage of female smokers (70%) followed by Egypt (64%), Palestine (62%), the United Arab Emirates (61%), Jordan (60%), Qatar (54%), Bahrain (54%), and Saudi Arabia (53%). In contrast, Kuwait (53%) and Oman (69%) had a higher proportion of men than women who smoked during the lockdown (Figure 2).
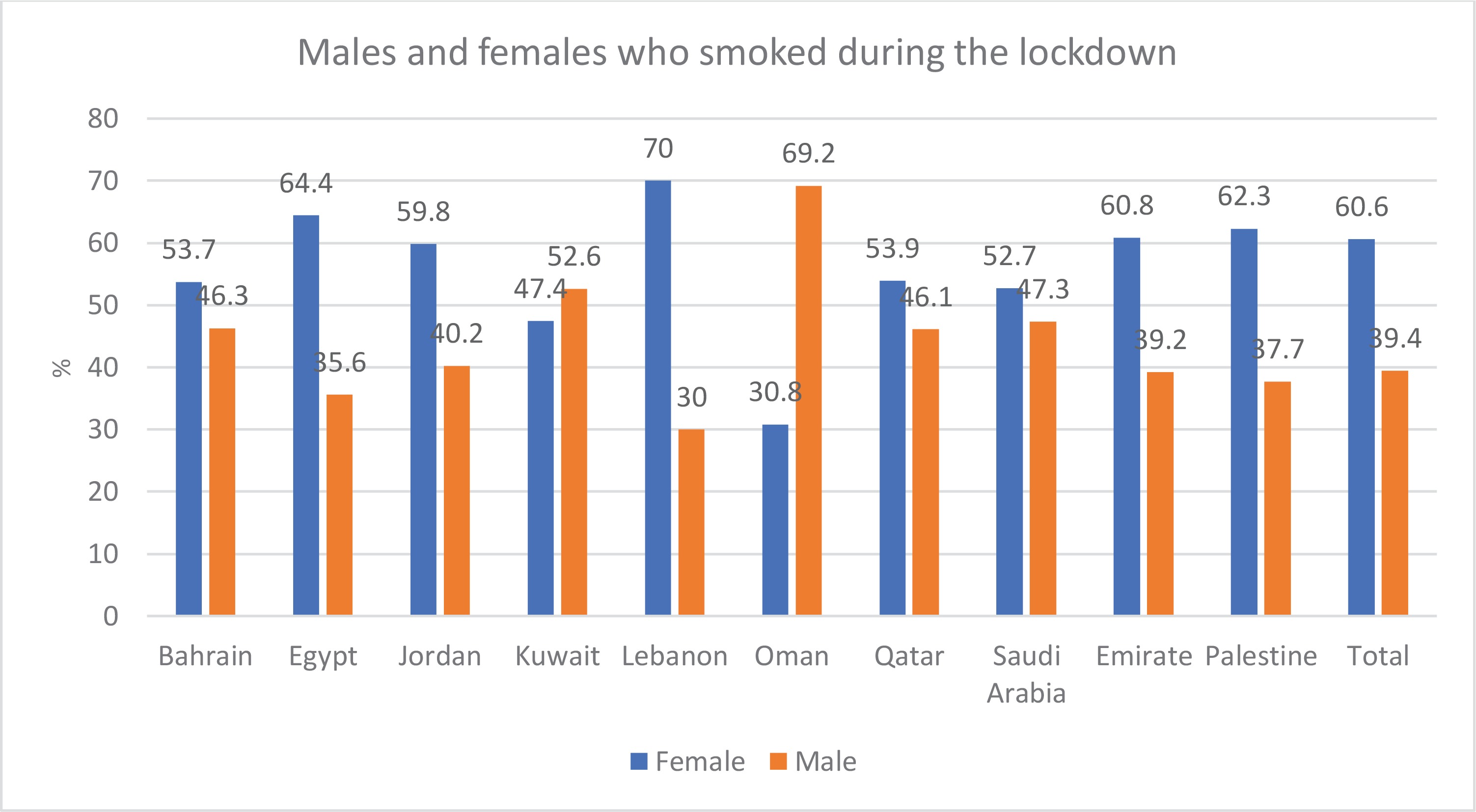
By comparing the percentages of female smokers before and during the lockdown in the 10 Arab countries, it was found that, except for Egypt and Oman, the percentage of female smokers before the lockdown was higher than the percentage of female smokers during the lockdown. In Egypt, the percentage of women who smoked before the lockdown was 64.2% and slightly increased during the lockdown to 64.4%. In Oman, the rate of females who smoke increased from 25% before the lockdown to 31% during the lockdown. In contrast, the data show that, with the exception of Egypt and Oman where the percentage of males who smoke was higher before the lockdown and decreased during the lockdown, the percentage of males who smoke before the lockdown increased during the lockdown (Figures 1 and 2). Results across the 10 Arab countries showed that males had a significant difference from female, before and during the lockdown (p<0.05).
Prevalence of smoking by age
Table 2 provides information on the various age categories of smokers in the 10 Arab countries before and during the lockdown. In Bahrain, Jordan, Lebanon, Oman, Qatar, Saudi Arabia, the United Arab Emirates, and Palestine, most smokers are between the ages of 20 and 29 years. In Kuwait, most smokers are aged between 40 and 49 years. In Egypt, the majority of smokers are 50 years of age or older.
Table 2
Sociodemographic characteristics, work status, and BMI, before and during COVID-19 among participants of 10 Arab countries, 2020 (N=12433)
Overall, the percentage of smokers aged between 20 and 29 years decreased during the lockdown in Bahrain, Qatar, Saudi Arabia, and the United Arab Emirates. Similarly, in Egypt, the number of smokers aged ≥50 years decreased during the lockdown. On the other hand, the percentage of smokers aged between 20 and 29 years increased in Jordan, Lebanon, and Oman during the lockdown. Also, in Kuwait, the number of smokers aged ≥50 years increased during the lockdown.
In conclusion, smokers in Jordan, Lebanon, Oman, and Kuwait increased their smoking during the lockdown. In contrast, most smokers in Bahrain, Qatar, Saudi Arabia, the United Arab Emirates, and Egypt decreased their smoking. In Palestine, smokers aged 20–29 years show a consistent percentage before and during the lockdown. In Egypt, Jordan, Lebanon, Qatar, Saudi Arabia, and the United Arab Emirates, data showed that the second and third age groups (20–29; 30–39 years) had significant difference at p<0.05.
Prevalence of smoking by education level
According to Table 2, most participants who smoked before and during the lockdown in Bahrain, Egypt, Jordan, Kuwait, Oman, Qatar, Saudi Arabia, the United Arab Emirates, and Palestine had Bachelor’s degrees. In Lebanon, most smokers had a high school diploma or less. The findings indicate that, during the COVID-19 pandemic, smoking rates among those with a Bachelor’s degree increased in Egypt, Oman, Saudi Arabia, and Palestine while decreased in Bahrain, Jordan, Kuwait, and the United Arab Emirates. In Lebanon, smoking increased during the lockdown. In Egypt, Kuwait, Lebanon, and Saudi Arabia, the data showed a significant difference in the education level of smokers before and during the lockdown (p<0.05).
Prevalence of smoking by working status
Before the lockdown, the prevalence of unemployment among the overall sample was 60%. This percentage increased to 69% during the lockdown. Countries that showed the highest increase in the unemployment rate were Jordan (82%), Kuwait (72%), Lebanon (69%), and Palestine (61%) (Table 2).
Prevalence of smoking by BMI
Before the lockdown, Oman (33%), Bahrain (28%), and Qatar (26%) had the highest rates of obesity among smokers. During the lockdown, Bahrain (32%), Qatar (31%), and Oman (25%) had the highest rates of obesity among smokers. As observed in the data results, the percentage of obesity among smokers increased during the lockdown in both Bahrain and Qatar, while it decreased in Oman. Before the lockdown, the percentage of overweight smokers was highest in Egypt (37%) followed by Qatar (36%) and Oman (33%).
In addition, during the lockdown, the percentage of smokers who were overweight was highest in Egypt (43%), followed by the United Arab Emirates (39%) and Qatar (38%). According to the data, while the percentage of overweight among smokers in Egypt and Qatar increased slightly during the lockdown, the overweight among smokers in the United Arab Emirates increased significantly. Before the lockdown, the percentage of overweight among smokers in the United Arab Emirates was 28%; during the lockdown, it increased to 39%, indicating a significant increase in weight among smokers. The data reveal a considerable change in BMI between before and during the lockdown in Jordan, Lebanon, Oman, and Saudi Arabia, the overweight and obese participants had significant differences from normal BMI participants.
Binary logistic regression analysis
Logistic regression was performed to ascertain the effects of the COVID-19 pandemic on smoking by age, gender, country of residence, physical activity levels, and participants working status. Table 3 shows the binary logistic regression analysis of smoking by sociodemographic variables. The logistic regression model was statistically significant by age, gender, education level, country of residence, work status, and watching TV activity. The regression model revealed an increase in smoking by age (20–29 and 30–39 years) during the COVID-19 lockdown compared to smoking before; the estimated odds ratio between smoking before and during the lockdown for the age groups 20–29 and 30–39 years, ranged 1.29–1.41 and 1.39–1.52, respectively. Furthermore, the results show increases in the odds ratio between smoking before and during the COVID-19 lockdown by gender, country of residence (Jordan, Lebanon, and Palestine), and working status. An interesting finding was a decrease in the smoking rate during the COVID-19 pandemic compared with smoking before the pandemic, according to TV watching activity.
Table 3
Binary logistic regression analysis of smoking before and during COVID-19 lockdown by age, physical activity, country, education level, gender, work status, and watching TV, 2020 (N=12433)
DISCUSSION
This cross-sectional study offers information about the effects of COVID-19 on cigarette and waterpipe smoking among people by gender, age, educational level, and BMI, in the 10 Arab countries that participated in an online survey following the lockdown to stop the spread of COVID-19 and lower the prevalence of smoking among people living in these countries.
According to our data, smoking had generally decreased during the lockdown in most Arab countries. However, it remained high in Lebanon, Jordan, and Palestine; this might be related to the economic stress experienced in these low-income countries where people were either unemployed or, at most, receiving half their typical salary for more than four months; the lockdown posed significant difficulties and limitations. This finding was similar to that of a study conducted in the middle African region21. Smoking was one of the psychological responses used by young adults to deal with the stress and anxiety associated with meeting their basic needs. One study found that smoking was significantly associated with stress and psychological distress among adolescent refugees in Lebanon, Jordan, Palestine, and Syria28.
Additionally, a study conducted by Chezhian et al.29 revealed that stress was one of the contributing factors that led people to smoke in general situations. Unemployment was found in our study to increase smoking during the lockdown and to be associated with smoking30. Furthermore, based on our study results, Lebanon shows a high percentage of smoking among females and males before and during the lockdown. According to Gulf News, Lebanon has ranked third in the world for the highest tobacco consumption per capita and that smoking is considered one of the cultural practices in Lebanon31. Additionally, a study reveals that due to Lebanon’s extensive tobacco growing, the availability and access to tobacco is easier and the average monthly consumption of cigarette packs is 12.4 packs (2008–2009 study), which exceeds that in Jordan (3.7 packs) and Syria (4.4 packs)32. During the pandemic, people also experience higher fear, higher boredom, and higher anxiety from the COVID-19 disease spread and lockdown, as found by Haddad et al.17 in a study in Lebanon.
Interestingly, in most of the 10 Arab countries, except for Oman, Qatar, and Kuwait, the smoking rate among women was greater than that of men both before and during the lockdown, with a higher odds ratio during the pandemic lockdown. This result was inconsistent with a study by Kashyap et al.33, and might be due to the higher percentage of women who participated in their study. Other studies show that men smoke more often than women, which increases the susceptibility and severity of COVID-19 among men rather than women34. However, our study’s findings may be explained by the fact that Arab women were not adapting to the presence of men at home all the time, as well as by the transition of children to online education, which added more pressure and stress on women. In addition, based on a UN women’s organization35, the reported cases of violence against Arab women increased during the lockdown; which showed that, after considering all the economic, social, and cultural views of Arab countries, the reported violence (physical, psychological, and sexual) during the lockdown was significantly higher than previously. Due to the restrictions on movement during the lockdown, women tend not to ask for assistance and receive little help from even their extended families. Given the challenging circumstances they endure and the fact that many women are forced to live with their abusers in the same house day and night, smoking may be the only coping mechanism they have access to. Although smoking was linked to violence in earlier research before the pandemic, our study may be the first to connect smoking with gender during the lockdown. The earlier studies found that women who experience violence increase their smoking behavior36,37.
Education was one of the most important results that our study showed. Despite having a higher level of education (at the university Bachelor’s level), smoking rates among students increased during the lockdown in most studied countries. Formal education level was positively associated with the cessation of smoking and not smoking in previous studies38.
Age was another factor we examined in our study, and we found that younger ages, between 20 and 29 years, may be associated with economic stressors or free time during the lockdown. According to our research, Egypt had the highest prevalence of smokers among those aged ≥50 years, with a rate of 31.8%. This result was similar to a cross-sectional study conducted in Egypt where the prevalence rate was 25.3%39. Therefore, increasing the percentage of active smokers among the elderly might increase the Case Fatality Rate in Egypt, as mentioned in a study that COVID-19 attacks the elderly more aggressively than children40. Furthermore, tobacco smokers are at high risk of severe COVID-19 due to chronic lung diseases, weak immunity, and cross-infection, as the smokers share devices between them with poor hygiene practices.
Regarding obesity and overweight among the smokers before and during the lockdown, the highest percentage of obese smokers before the lockdown was in Oman (33%), followed by Bahrain (28%) and Qatar (26%), whereas, during the lockdown, the percentage of obese smokers was highest in Bahrain (32%) followed by Qatar (31.3%) and Oman (25%). Results revealed that most Gulf Cooperation Council countries have high rates of obesity among both genders, which may increase the burden of disease in the future. In a study by Radwan et al.18, the lockdown in the UAE resulted in higher food consumption and lower levels of physical activity. Therefore, an increase in weight is experienced with an increase in smoking frequency. These factors can increase vulnerability of being infected by COVID-19 and worsen the severity of the disease, which was consistent with our study. The percentage of overweight smokers in the UAE before the lockdown was 28%, whereas during the lockdown it increased to 39%. Obesity and overweight did not increase in low-income countries during the lockdown since food consumption did not rise, and in some cases, people suffered from a lack of resources.
Interestingly, our study shows a significant association between watching TV and a decrease in smoking behavior during the lockdown, as the more hours spent watching TV, the lower the odds ratio with smoking during the lockdown. During the lockdown, people face fear, loneliness, and eagerness to follow up on the pandemic distribution and lockdown updates; watching TV was one of the strategies to deal with all those feelings found in other studies19,20. In addition, to the fact that people understand the effect of second-hand smoking on infectious diseases such as COVI-19, smoking while watching TV is reduced, and people tend to relapse from smoking while watching TV. Since they spend more time at home watching TV, simultaneously the smoking rate will be lower19.
Strengths and limitations
When interpreting the results, it is necessary to consider the study’s strengths and limitations. The diversity of the sample from 10 Arab countries is a study strength. This study is the first, that we are aware of, that attempts to quantify changes in smoking practices in numerous Arab countries. The results of this study may thus be applied to the entire population of the 10 Arab countries during the lockdown. Besides the strengths of this study, it is not without limitations. One of the limitations is related to the data collection before and during COVID-19 based on self-report, which might have resulted in participant recall bias. Another limitation is associated with the comparison of the current study with other similar studies by using different methods to measure smoking and assess screen time, making direct comparisons with results and conclusions difficult. Using a cross-sectional study design limits ascertaining causality relationships. Moreover, the study’s convenience sampling might limit generalizability. Cross-cultural differences between countries are considered another limitation for interpretations and comparisons.
CONCLUSIONS
Internationally, many strategies have been advocated to prevent the spread of COVID-19, including social distancing, strict hygiene, and extreme circumstances like lockdown. A lockdown was implemented during COVID-19 as a quick action to limit the spread of the disease. However, this action had many unintended consequences, some of which were obvious, like economic issues, and others not so obvious, like smoking, female smoking rates rising, and increased food consumption and obesity.
Special attention must be paid to illness prevention and health promotion, with a focus on smoking and diseases like COVID-19 and other respiratory conditions. During the lockdown, or other infection control in the event of a pandemic, a healthy lifestyle must be supported and promoted. Better preparedness and planning for health promotion campaigns must accompany any lockdown strategies to combat infectious diseases in the future, including reducing smoking and encouraging a healthy lifestyle.